Published: July 2026
Read time: 4 mins
Published: July 2026
Read time: 4 mins
More than eight billion people live on Earth. Fewer than 700 have ever left it to venture into space. Robert Thirsk is one of them.
Long before Robert became an astronaut with the Canadian Space Agency (CSA), he was a young boy living in British Columbia watching the Apollo moon landing on television with his family. When the broadcast ended, he ran outside to look up at the moon. He was captivated. The astronauts who had travelled there seemed impossibly brave. From that moment, he dreamed of following in their footsteps.
Years later, he would do exactly that.
“It was at that moment I realized I had fulfilled a childhood dream.”
— Robert Thirsk
In 1996, Robert first launched into space and spent 17 days aboard Space Shuttle Columbia. Then in 2009, he spent 6 months in orbit, floating weightless aboard the International Space Station and looking down on Earth from a perspective few people will ever experience. He still remembers the first time he saw the sun rising across the Atlantic Ocean from above.
“It was at that moment I realized I had fulfilled a childhood dream,” said Robert.
But years after returning from space, an unexpected problem here on Earth began affecting his daily life.

More than a pinched nerve
At first, Robert assumed it was a pinched nerve. Whenever he gazed ahead or to his right, numbness and tingling would radiate from his right shoulder down his arm and into his fingers. The sensation disappeared almost immediately when he turned his head the other way. But every time he looked to his right again, it returned.
He thought it would resolve on its own with the help of a few exercises. Instead, it persisted, and the symptoms began interfering with everyday activities such as driving and watching television. As time passed, he also noticed a loss of strength in his upper arm. For someone who has maintained an active lifestyle and pushed the limits of human performance — as an engineer, a physician, and an astronaut — the loss of function was difficult to accept.
“I couldn’t go through the rest of my life only looking to my left,” said Robert.

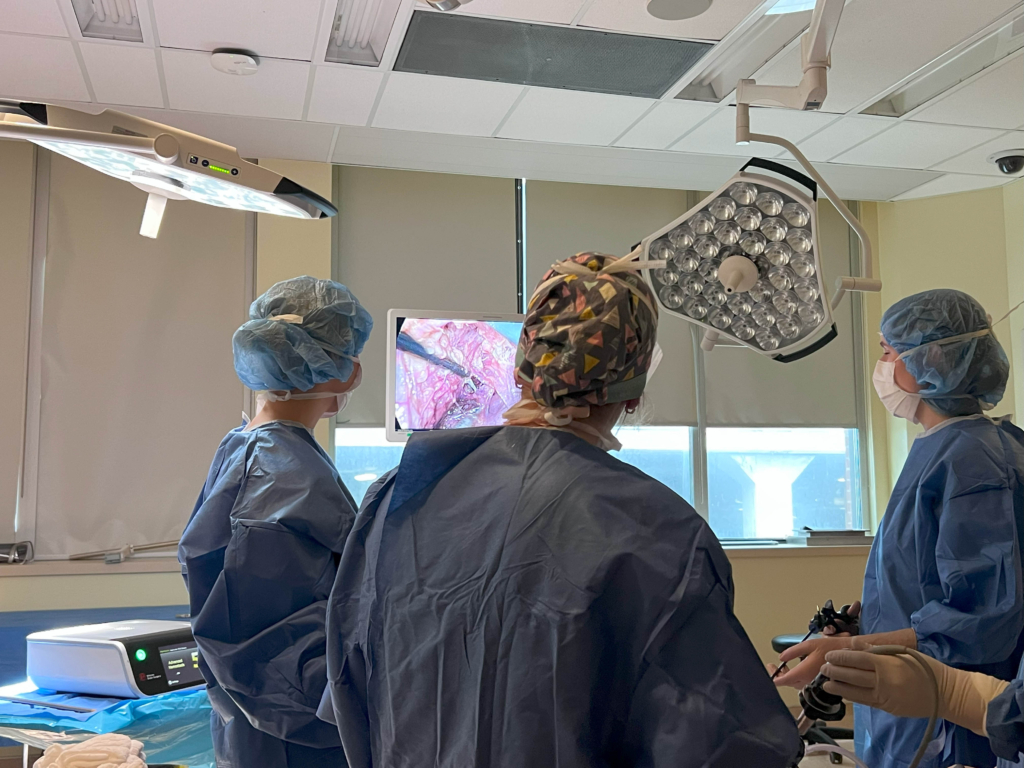
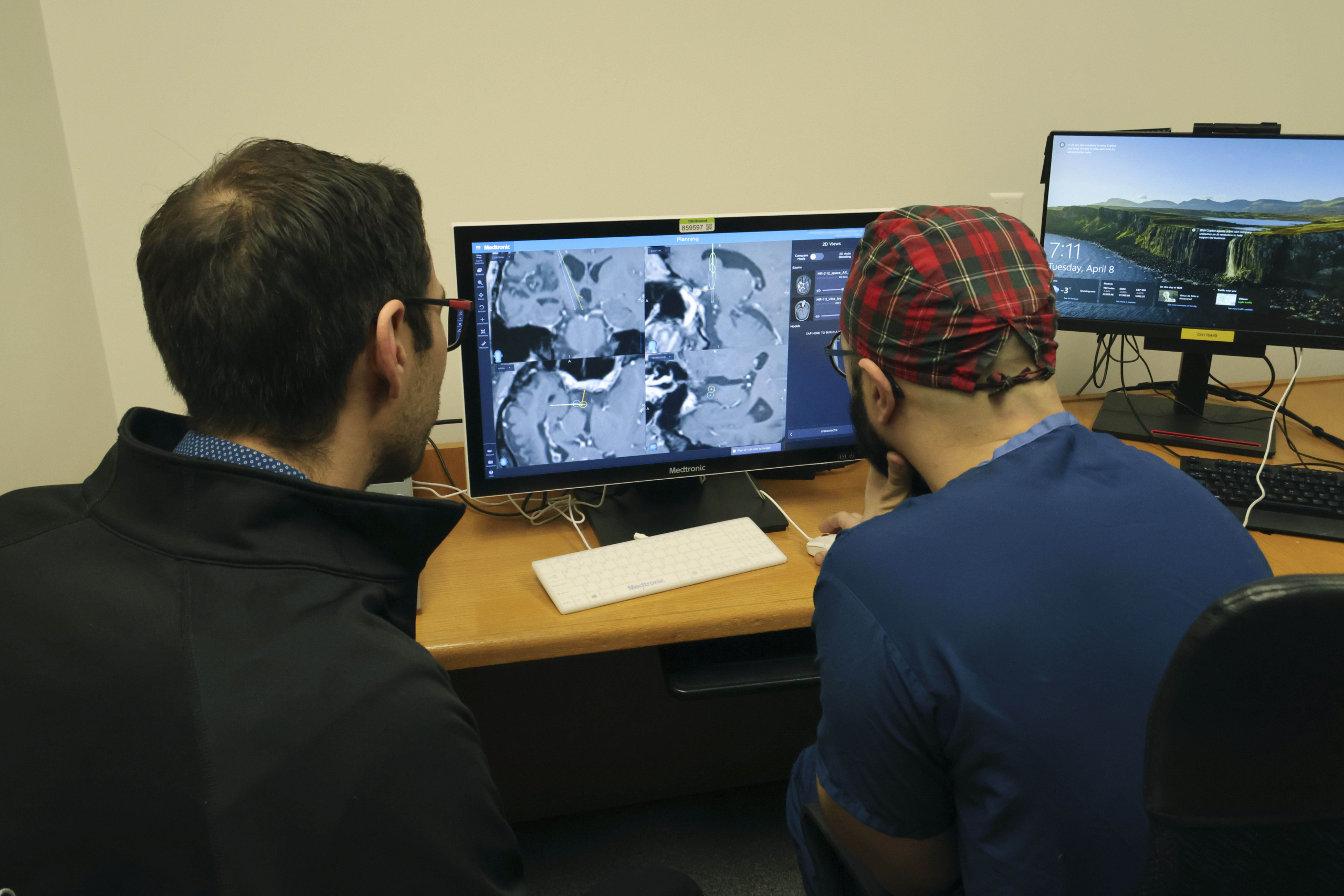
A novel approach to spine surgery
As the symptoms worsened, Robert was referred to Dr. Safraz Mohammed, neurosurgeon at The Ottawa Hospital. Imaging, including X-rays and an MRI, revealed osteoarthritis in his cervical spine. A degenerated disc at the C5-C6 level had herniated and was compressing a nerve root in Robert’s neck, triggering the numbness, tingling, and weakness that was disrupting his life.
The diagnosis brought an important decision. Traditionally, many patients with this type of condition undergo spinal fusion surgery, a procedure that permanently joins two vertebrae together. While highly effective at relieving pain and stabilizing the spine, it eliminates movement at that level of the spine. For Robert, maintaining the mobility of his neck was essential.
Dr. Mohammed believed Robert could benefit from a novel procedure known as artificial disc replacement. Unlike spinal fusion, artificial disc replacement uses an implanted device designed to preserve movement in the neck while relieving pressure on the affected nerve.
Not every patient is a candidate for the procedure, but Robert’s overall health, active lifestyle, and strong bone quality made him an excellent fit.
“Artificial disc replacement allows us to treat the source of the problem while preserving motion in the neck,” said Dr. Mohammed. “For patients, it can provide excellent symptom relief while helping them maintain the active lifestyle they enjoy.”
It also meant Robert could benefit from expertise available at only a few hospitals in Ontario. Dr. Mohammed is among the region’s leading spine surgeons trained to perform the highly specialized procedure. In fact, he is helping train other surgeons to offer it across the province.
Prepared for launch … and surgery
For Robert, the decision felt surprisingly familiar. Throughout his career as an astronaut, he learned that extraordinary outcomes depend on extraordinary teams. After discussing the risks and benefits of each option with Dr. Mohammed, Robert felt confident he was in the right hands and wanted to move forward with the innovative procedure.
Despite the complexity of the operation, he wasn’t nervous on the day of surgery. His years of astronaut training taught him that trust matters when outcomes depend on a highly skilled team. In many ways, the feeling reminded him of walking out to the launch pad before both of his space missions. “You might think astronauts would be nervous at that moment,” said Robert. “But actually, we’re reflecting on the quality of our training as well as the preparation of our ground support team. Prior to both launches, I had complete confidence in the abilities of myself, my crew mates, and the ground team to accomplish our ambitious mission objectives.”
That same sense of confidence carried him into the operating room.
Speedy recovery
The surgery was completed successfully, and Robert felt the results immediately. When he woke up after surgery, the symptoms that had disrupted his life were gone. “I noticed right away the numbness and tingling had disappeared,” said Robert. “How remarkable!”
What impressed him just as much was the speed of recovery. Even after such a complex operation, he spent just one night in hospital before returning home.
Within a few months, Robert had returned to all of the activities he previously enjoyed, moving freely without experiencing any symptoms.

What happens to the body in space?
While The Ottawa Hospital helped restore Robert’s mobility and quality of life, researchers at our hospital have spent years studying how spaceflight affects the human body.
For decades, Dr. Guy Trudel, a rehabilitation physician and senior scientist at The Ottawa Hospital, has been at the forefront of that work. His internationally recognized research has helped the Canadian Space Agency and scientific partners around the world better understand how prolonged exposure to weightlessness changes muscles, bones, joints, and the spine.
Much of his work combines clinical research with experiments on astronauts in space and space analog studies. In the studies, on Earth, healthy volunteers participate in controlled bed rest experiments that simulate the effects of microgravity. Researchers carefully track changes in muscle strength, bone density, circulation, and the spine using advanced imaging and physiological testing.
“The body adapts remarkably well to space, but returning to gravity places new demands on bones, muscles, and the spine.”
— Dr. Guy Trudel
In space, astronauts grow taller as spinal discs expand without the constant pull of gravity. Many experience back pain during missions, and research suggests spaceflight may increase the risk of spinal problems after returning to Earth.
“We know that spaceflight affects the musculoskeletal system in many ways,” said Dr. Trudel. “The body adapts remarkably well to space, but returning to gravity places new demands on bones, muscles, and the spine.”
His work has also led to important discoveries about changes in bone marrow. The MARROW study, published in Nature Medicine, led to a better understanding of space anemia, a condition which affects astronauts after spaceflight. His team is now entering the next phase of research through the SPARK study, which will build on earlier findings identified through MARROW, with data collected from astronauts before, during, and after spaceflight.
Meet researcher and physician Dr. Guy Trudel
The impact of this research also extends beyond space exploration.
“The same changes we see in astronauts can also occur in patients who are immobilized for long periods of time,” said Dr. Trudel. By studying how the body responds to weightlessness, researchers are gaining insights that could help improve care for patients on Earth who spend long periods of time in bed due to illness or injury. Those discoveries could help identify new ways to prevent muscle loss, preserve bone health, and improve recovery for patients.
Whether Robert’s spinal ailment was connected to his time in space is impossible to know with certainty, but his experience highlights two areas where The Ottawa Hospital is making a difference: delivering leading-edge care for patients today and while advancing research that could help shape the future of human space exploration.
Life without limitations
Today, Robert is back to the active lifestyle he loves. Looking back, he is grateful for the expertise, innovation, and care that helped restore his mobility. For Robert, the experience was a reminder that exploration takes place at a variety of frontiers, including surgical and scientific.
Whether advancing our understanding of the human body through spaceflight research or offering cutting-edge surgical options closer to home, The Ottawa Hospital continues to push the boundaries of what is possible for patients in Ottawa and far beyond.