New TD Artificial Intelligence in Medicine (AIM) Hub to transform healthcare in Ottawa and around the world
Category: Creating Tomorrow
March 1, 2022 – Through a $2-million donation from TD Bank Group (TD), The Ottawa Hospital will create the new TD Artificial Intelligence in Medicine (AIM) Hub that will accelerate the development and use of artificial intelligence (AI) in healthcare. AI has the potential to transform the prevention, diagnosis, and treatment of chronic diseases such as diabetes, kidney disease, cancer, heart disease, and brain conditions. It could be a game changer for patients not only in Ottawa but also across Canada and around the globe.
Dr. Doug Manuel, senior scientist at The Ottawa Hospital and distinguished professor at the University of Ottawa, will lead this innovative project. Dr. Manuel explained the TD AIM Hub will build on our world-leading experience developing mathematics models or algorithms to not only improve diagnosis and treatment but also predict potential issues and outcomes. “From a simple technology perspective, complex data and algorithms currently take nine months to three years to develop and implement. We are proposing an aligned model in which this cycle will take only days.”
Traditionally, this has been a huge gap, with the vast majority of AI innovations never progressing beyond the earliest stages of research. Dr. Alan Forster, Executive Vice-President, Chief Innovation and Quality Officer, and senior scientist at The Ottawa Hospital explained how this platform would help bridge this gap. “The TD AIM Hub will engage patients and their loved ones directly in the development of AI tools from the earliest stages to ensure the patient experience is front and centre. It would be a collaborative effort between patients, physicians, scientists, and programmers. Importantly, we will evaluate the impact of the AI tools to improve outcomes that matter most to patients.”
“At TD, we are thrilled to provide funding to The Ottawa Hospital to help extend innovative AI technology capabilities and advance quality healthcare in the region,” said Tara-Lynn Hughes, Senior Vice President, TD Bank Group. “Through the TD Ready Commitment, the Bank’s corporate citizenship platform, this important initiative will help patients living with cardiac conditions, cancer, and other chronic diseases access equitable and personalized care.”
The TD AIM Hub will ensure that our hospital is ideally positioned to take advantage of the incredible potential of artificial intelligence, according to Dr. Duncan Stewart, Executive Vice-President, Research and senior scientist at The Ottawa Hospital. “In the past, it has been a challenge to implement increasingly complex algorithms into practice. This new virtual Hub will revolutionize our ability to use AI to transform the practice of medicine. I am thrilled that TD has had the foresight and generosity of spirit to support this innovative initiative to harness complex data to improve healthcare.”
The TD AIM Hub will have three capstone chronic disease projects including multiple chronic disease prevention, end-stage renal disease, and degenerative neurologic conditions. This platform will build on our hospital’s track record of world-firsts, including the first and largest hospital data warehouse in Canada, the first hospital-wide “synthetic” data program in Canada, and one of the most comprehensive sets of health calculators and predictive algorithms in the world, with more than 2 million users in 200 countries.
About The Ottawa Hospital:
The Ottawa Hospital is one of Canada’s top learning and research hospitals, where excellent care is inspired by research and driven by compassion. As the third-largest employer in Ottawa, our support staff, researchers, nurses, physicians, and volunteers never stop seeking solutions to the most complex healthcare challenges.
Our multi-campus hospital, affiliated with the University of Ottawa, attracts some of the most influential scientific minds from around the world. Our focus on learning and research leads to new techniques and discoveries that are adopted globally to improve patient care.
We are the Regional Trauma Centre for eastern Ontario and have been accredited with Exemplary Standing for healthcare delivery — the highest rating from Accreditation Canada. We are also home to world-leading research programs focused on cancer therapeutics, neuroscience, regenerative medicine, chronic disease, and practice-changing research.
Backed by generous support from the community, we are committed to providing the world-class, compassionate care we would want for our loved ones.
For more information about The Ottawa Hospital, visit ohfoundation.ca.
Update June 2026:
We are deeply saddened to share that Owen passed away on May 31, 2026. Owen survived cancer three times and was a successful, early recipient of our hospital’s made-in-Canada CAR T-cell therapy. He was a proud advocate for the program, and we’re so grateful he shared his story with us. Our deepest condolences to this family.
Originally published: January, 2022
When Owen Snider faced the news that his lymphoma had returned for the third time in ten years, he knew his options were running out. But a transformational new treatment known as CAR-T therapy gave him renewed hope. The Ottawa Hospital was recruiting patients for a clinical trial investigating a made-in-Canada approach to this cutting-edge treatment. He just needed to qualify for the trial.
In 2010, Owen was diagnosed with large B-cell lymphoma. In his early 60s at the time, he went through a chemotherapy treatment known as R-CHOP. For most people, it lasts 18 weeks. “It was a rigorous treatment. I got through it okay and was six years clear, but then it came back — the lymphoma returned in 2016,” says Owen.
When the cancer returned, his care team at The Ottawa Hospital vetted him for a stem cell transplant. By the summer of that year, he went through what he called an intensive program using his own stem cells. A high dose of chemotherapy was used to remove harmful immune cells in preparation for the transplant of his own healthy cells. “It’s pretty brutal, and after two or three months of wishing maybe I wasn’t around, things improved. I was clear for another four years.”
“I was given five or six months to live. My wife and I were downhearted with that news.”
— Owen Snider
Lymphoma returns for a third time
Following his stem cell transplant, Owen remained healthy for four years, enjoying retirement at his home in a beautiful, wooded area near Calabogie, where he lives with his wife, Judith Snider. But then Owen faced his biggest challenge yet when the lymphoma returned — again. This time, the diagnosis came in May 2020, in the midst of the pandemic. “I remember my oncologist saying they’ve done pretty much everything they could. I was given five or six months to live. My wife and I were downhearted with that news. I was basically going to be kept as comfortable as possible for six months,” remembers Owen.
Judith and Owen Snider kayaking.
However, one week later Owen received a lifeline. His oncologist called to say a CAR-T therapy clinical trial had opened at The Ottawa Hospital — a Canadian first. They wanted to see if he would be a good candidate. Throughout June of 2020, he went through a battery of tests and scans to see if he qualified for the trial.
“This type of immunotherapy research is groundbreaking, and it’s never been done in Canada before.”
– Dr. Natasha Kekre
By mid-June, Owen got the green light. He was a candidate for the clinical trial, and didn’t hesitate to enroll. “I either participate in the trial or I lie around here for four or five months waiting for the end. Which choice would you have made? The positive way to put it is that I was very excited to be a part of the trial. We’re the kind of people where the glass is always half-full,” explains Owen.
CAR T-cell therapy is a type of immune therapy that is an emerging biotherapeutic treatment that harnesses the power of a patient’s own immune cells, known as T-cells, to treat their cancer. T-cells play a critical role by killing abnormal cells, such as cells infected by germs or cancer cells. In some cancers, like lymphoma or leukemia, cancerous cells become invisible to the T-cells that are meant to kill them. In CAR-T therapy, the T-cells are collected and reprogrammed in the lab to recognize and destroy the cancerous cells.
Dr. Natasha Kekre is a hematologist and associate scientist at The Ottawa Hospital. She is leading the development of Canada’s first CAR-T research platform in collaboration with the BC Cancer Centre. “This type of immunotherapy research is groundbreaking, and it’s never been done in Canada before. This is a therapy that uses a patient’s own immune system. It’s personalized medicine — it’s very individualized to each patient,” explains Dr. Kekre.
The Ottawa Hospital is one of the first hospitals in Canada to participate in nationally-led CAR-T trials, and as one of Canada’s top research and treatment centres, the hospital is ideally positioned to play a lead role in bringing an innovative CAR-T research program to Canada, and to Canadian patients.
Going for the Pac-Man effect
In late June 2020, Owen went through apheresis which is the process of withdrawing the T-cells in his blood. “They put an IV in my right arm, and ran the tubing through the machine, and the machine processes the blood and pumps it back through the tubing into my other arm. I lay there on the bed for three or four hours, without moving I should add.”
“It’s just like Pac-Man, the modified T-cells ran around in my blood stream, chomping away at the lymphoma.”
– Owen Snider
Those T-cells were then sent to a lab in BC, re-programmed, and then returned to our hospital two weeks later. Then the T-cells were re-administered just like a blood transfusion. “It allows for that new immune therapy in these cells to go and find the patient’s cancer cells, attack them, and kill them. And it also stimulates the immune system in that patient to further go attack and fight their cancer,” explains Dr. Kekre.
On July 2, Owen received a PICC line and then went through three days of chemotherapy. Four days later he was re-injected with his T-cells and they got to work. “It’s just like Pac-Man, the modified T-cells ran around in my bloodstream, chomping away at the lymphoma.”
His re-programmed T-cells were specifically looking for cancer cells to kill. Owen would need to wait to find out if it was working.
Owen Snider
Did the CAR T-cells therapy work?
One month later, Owen and Judith received some exceptional news. “At my check-up 30 days after getting my T-cells back, I was almost clear of cancer. The scan showed that there was almost nothing left. I was gobsmacked,” he says.
By the three-month mark, Owen says he was as “clean as a whistle.” Eighteen months later, there is still no sign of lymphoma.
For Dr. Kekre, giving patients like Owen new hope for the future is what inspires her. “For the first time, I think in a long time, Owen felt that the lymphoma might actually be disappearing. He’s had multiple scans since then that show the same thing. And so now, I think he’s starting to believe it. And I think that’s the reality of why I do this, because patients like him who had no options before, could soon have the option of CAR-T therapy. That’s what happened for Owen and that’s what we hope will happen for many more patients,” says Dr. Kekre.
Dr. Natasha Kekre and Owen Snider. Owen was treated for lymphoma as part of a CAR-T clinical trial.
What’s next for the clinical trial?
Dr. Kekre and her team are monitoring all patients enrolled in the trial and published preliminary results in June 2022. The purpose of the clinical trial is to provide proof to Health Canada this therapy is safe. “The reality is that we have a data safety monitoring board, which watches for the safety of the trial, and they’ve had no concerns. So, from a safety point of view, we’re very happy with the trial. And that’s why we are still open and we’re still able to enroll more patients,” explains Dr. Kekre.
Download Pulse Podcast today to hear Dr. Natasha Kekre share more about her game-changing clinical trial.
Why is The Ottawa Hospital unique in its CAR-T therapy?
CAR-T therapy needs to be individually manufactured for each patient using the patient’s own cells combined with large amounts of highly pure virus to deliver the chimeric antigen receptors (CAR) gene. The Ottawa Hospital’s Biotherapeutics Manufacturing Centre is ideally positioned to manufacture the clinical grade virus needed to create CAR T-cells for clinical trials. In fact, we have the only facility in Canada that has produced this kind of virus for clinical trials.
The hope is that one-day CAR T-cell therapy may also be a treatment for a variety of cancers. “The world is watching us,” explains Dr. Kekre. “We’ve had a lot of attention from Denmark, and a few other European countries are reaching out. They believe in a system similar to ours, where patients all have the right to access healthcare. If CAR T-cells are here to stay, they have to be done in a sustainable approach for our patients. And that’s a big part of what we are building — this is only the beginning. And that’s what people are looking at us to see how we do it.”
“Without philanthropy, we wouldn’t have a Biotherapeutics Manufacturing Centre or a Methods Centre at The Ottawa Hospital, and we wouldn’t be able to do innovative clinical trials like this.”
– Dr. Natasha Kekre
This made-in-Canada CAR T-cell research platform will give Canadian patients more access to innovative clinical trials. “Canadian cancer patients shouldn’t have to wait for the research to be done elsewhere but be able to participate in innovative clinical trials here at home,” says Dr. Kekre.
Grateful for each day and philanthropic support for research
Today, Owen appreciates each day and a good quality of life thanks to the clinical trial. He feels strong and can’t wait for the day when he and Judith can travel again — grateful for the lifesaving research. “It was an honour and a privilege to be chosen for the trial.”
He also credits the extraordinary care team and those special moments when he visited the hospital. “I can tell you that I always felt more than comfortable. I felt encouraged by anyone I met. The team on 5 West as we know it, is wonderful. I had an occasion to go back there last spring, and it was like walking back into Cheers — everybody knows your name.”
As a longtime supporter of The Ottawa Hospital, and to see philanthropy play an important role in making this clinical trial a reality, he’s an even bigger advocate for encouraging support for our hospital. “All I can say is that the core funding of hospitals doesn’t provide for some of the innovative and cutting-edge things that go on, or maybe some really specialized piece of equipment. And that’s where the community donor can help and contribute to that effort.”
Owen and Judith Snider.
For Dr. Kekre, philanthropy provides the spark for clinical trials like this, and can help to keep them moving forward. “Without philanthropy, we wouldn’t have a Biotherapeutics Manufacturing Centre or a Methods Centre at The Ottawa Hospital, and we wouldn’t be able to do innovative clinical trials like this. We need this kind of research to get to a place where all Canadians can benefit from these therapies. Without philanthropy, we would never get there.”
And to Dr. Kekre, her team, and their collective efforts to give more patients hope, Owen has a simple message: “Thank you. The whole program is outstanding.”
About the Canadian-Led Immunotherapies in Cancer (CLIC) research program
The CLIC research program, established in 2016, brings researchers, clinicians and patients from across Canada together to build Canadian expertise and capacity for innovation in the promising field of cellular immunotherapy for cancer, including CAR-T therapy. The first CLIC clinical trial launched in 2019 at The Ottawa Hospital and at BC Cancer, with support from BioCanRx, BC Cancer, The Ottawa Hospital Foundation and the Ontario Institute for Cancer Research. Core facilities and resources supporting CLIC include The Ottawa Hospital’s Biotherapeutics Manufacturing Centre, BC Cancer’s Conconi Family Immunotherapy Lab, the Ottawa Methods Centre and the Blueprint Translational Research Group. CLIC team investigators include Drs. Natasha Kekre, Harold Atkins, John Bell, Kevin Hay, Rob Holt, Brad Nelson, John Webb, Manoj Lalu, Kednapa Thavorn, Dean Fergusson, Justin Presseau and Jen Quizi.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Biotherapeutics, Cancer, Clinical Trials, Innovation and Technology, Patient Care, World-Leading Research
For decades, Paula Helmer’s lovely voice carried through the alto sections of several Ottawa choirs. But even after her death following a battle with breast cancer, Paula is still managing to be heard — maybe not through song, but through science.
“That’s what Paula was hoping for from all these clinical trials,” says Jeff Christie, Paula’s husband, “that it would move medical science forward.”
“That’s what Paula was hoping for from all these clinical trials, that it would move medical science forward.”
—Jeff Christie
Jeff and Paula met in university, both studying economics at the University of Waterloo, and both moving to Ottawa, Paula’s hometown, to work for the federal government in fulfilling careers that would span decades. All the while, Paula continued her passion for choral singing, with St. Timothy’s Presbyterian Church and the Ottawa Choral Society. But Jeff says it was family life that centred everything — children, grandchildren, travel, and the family cottage.
Paula (back row, fourth from right) in 2005 with members of the Ottawa Choral Society.
“Five years into retired life, it was discovered that Paula had cancer,” Jeff recalls.
It was a deadly form of breast cancer that had metastasized in her spine and was causing her considerable discomfort. Surgery removed the tumour but couldn’t eradicate the cancer, nor control the pain. That’s when Paula was introduced to Dr. Mark Clemons, a medical oncologist with The Ottawa Hospital.
“We came up with a multipronged plan to not only improve (Paula’s) pain,” Dr. Clemons explains, “but to get her disease back under control.”
“It was patently clear from the first meeting,” says Jeff, “that Dr. Clemons was very capable, competent, and wise. He gained our confidence the first time we met and the treatments he was suggesting for her, they were always so successful. How could you not love the guy?”
A passion to participate in clinical trials
Dr. Clemons is also the lead behind The Ottawa Hospital’s REaCT Program or Rethinking Clinical Trials, launched in 2014 with Dr. Dean Fergusson, senior scientist and Director of Clinical Epidemiology Program, and others. The aim of REaCT is to make enrollment in clinical trials easier, by involving cancer patients and their families every step of the way. Typically, only 3% of patients are involved in trials but with REaCT, that number is closer to 90% since the studies don’t involve extra visits or additional tests. Paula began participating in a series of clinical trials aimed at helping her, but also aimed at improving treatment options for future generations. Jeff says that was her driving ambition.
What is the REaCT Program?
The aim of the REaCT (ReThinking Clinical Trials) program is to make enrollment in clinical trials easier, by involving patients and their families every step of the way.
“Paula played an important role in advancing the treatment of patients across the world.”
— Dr. Mark Clemons
“It was really important to her, to both of us,” he says. “There are more treatments out there we haven’t found yet and we are going to find them through clinical trials. If you don’t participate, nobody gets the new treatments.”
Empowered and making an impact
More importantly, Jeff says, Paula’s participation in these clinical trials gave her a voice and made her an active participant in her treatment.
“Paula was always left with the impression that she was in the driver’s seat right beside Dr. Clemons. They listened to her, believed her.”
Dr. Clemons explains that one of the many clinical trials Paula participated in involved looking at how often bone agents should be given for patients with metastatic breast cancer. Traditionally, the treatment is delivered as an injection every four weeks, requiring patients to come to the hospital and spend prolonged periods away from home.
“Paula had a driving ambition to not only improve her own prognosis but also help with the knowledge being gained for future patients.”
— Dr. Mark Clemons
“Because of Paula and many other patients involved,” says Dr. Clemons, “we were able to do a trial that showed that an injection every 12 weeks was just as effective and was associated with fewer side effects.” It also added to Paula’s quality of life, allowing the couple to continue to visit the cottage and travel in between those 12-week injections.
“That was a great thing,” says Jeff. “The care we got was supportive of our lifestyle. It allowed us to travel as we had hoped to.”
Paula’s participation in a REaCT trial added to her quality of life, allowing her to continue to visit the cottage and travel with her husband, Jeff, in between 12-week injections.
Paula’s legacy lives on
Sadly, Paula lost her fight against cancer on February 18, 2021. But Jeff is continuing her work, spreading the word about REaCT among friends and colleagues, raising funds to support this critical work that is helping to shape better treatment options for cancer patients around the world.
“I’ve spoken about REaCT in my social circles,” Jeff explains. “I mentioned Paula has participated in at least dozens of clinical trials and benefited from them.”
“It’s fantastic that Jeff is continuing Paula’s legacy,” says Dr. Clemons. “Paula played an important role in advancing the treatment of patients across the world.”
It’s a role that she embraced with the same fervor she approached everything she did in life, whether as an economist, a wife, a mother, and yes, even a singer.
“There are more treatments out there we haven’t found yet and they are going to find them through clinical trials.”
— Jeff Christie
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Cancer, Clinical Trials, World-Leading Research
Darlene Kulig is an award-winning artist whose paintings are described as bold, joyous, and eye-catching. Born in Ottawa, Darlene now calls Toronto home and brings uniquely Canadian landmarks and landscapes to life through her semi abstracted, spirited art.
When Darlene’s nephew, Craig, passed away in 2016 at the age of 23 from a rare form of cancer, it was a devastating loss for her family. Craig’s father, Bruce Kulig, wanted to do something to keep his son’s memory alive, so he created a fundraising campaign — the Craig Kulig Memorial Fund with The Ottawa Hospital. When Darlene learned about the campaign, she wanted to use her art to have an impact.
Darlene began selling card sets featuring her art, with proceeds donated to our hospital. When the pandemic hit, her campaign took a different twist. She created beautiful masks, and once again a portion of the sales would support the memorial fund.
Today, Craig’s memory lives on through the countless people who have supported his memorial fund and the impact their philanthropy is having on cancer research. The research will help other patients and their families – just as Craig’s family had hoped.
Q: What inspired you to fundraise for The Ottawa Hospital?
A: In 2016, we lost our dear nephew Craig Kulig, at the age of 23, to an aggressive form of rare cancer. Craig received wonderful and compassionate care from the team of doctors and nurses at The Ottawa Hospital. Since Craig’s passing, it has been my brother Bruce’s goal to raise $100,000 in Craig’s memory.
As an artist and an aunt processing through my grief journey, I felt compelled to create a painting in memory of Craig. I painted Dragonfly Ascending into Twilight which depicts Granite Lake where Craig spent his youth. We donated the large giclee print of this meaningful painting and it now hangs in the oncology department at the hospital.
A memorial for Craig Kulig at Granite Lake with candle houses created by Craig’s sister Katrina.
Q: What is your fundraising all about?
A: Early in the pandemic, I was approached by BYOM, a mask manufacturer, to have my Canadian Landscape paintings printed as fine art face masks. Each artist that was approached was asked to align with a charity, so we created a beautiful line of adult and children’s face masks with all proceeds going to The Craig Kulig Memorial Fund. To date, we have raised over $16,000 through the sale of these masks. We also introduced a beautiful wall calendar and holiday boxed card sets featuring my art.
“As an artist and an aunt processing through my grief journey, I felt compelled to create a painting in memory of Craig.”
— Darlene Kulig
Q: How easy was it to set up a community fundraising event through our Foundation?
A: My brother Bruce set up The Craig Kulig Memorial Fund through The Ottawa Hospital Foundation. It has been a great experience working with their team to promote our masks, continue to raise money for Craig’s fund, and raise awareness for the leading research that is taking place at The Ottawa Hospital.
Q: What might you tell someone who is thinking about donating to The Ottawa Hospital?
A: I believe our fundraising efforts are going to make a difference. It is our hope that other individuals and families can and will have better outcomes. This takes time and much-needed donations. The Ottawa Hospital is a leading research centre that we are proud to be partnered with.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Cancer, Donors, World-Leading Research
For months, Mina King had been dealing with painful leg ulcers caused by atherosclerosis, a condition that restricts blood flow and can result in amputation if left untreated. As a lifelong musician, this prognosis would mean more than losing her legs, it would jeopardize her ability to play the piano — one of her greatest passions. But, a cutting-edge surgery technique at The Ottawa Hospital, the collaboration of our experts at the Limb Preservation Clinic (LPC), and ongoing virtual care to monitor her healing, kept Mina from missing a beat.
Ulcers: A persistent problem
When Mina first developed sores on both of her legs, she hoped they would eventually go away with time and care. But after almost a year and a half of appointments and regular monitoring at the LPC, things weren’t heading in the right direction.
“Bypass surgeries are very complex and take several hours to complete. Not every hospital is able to perform these surgeries because they’re so technically demanding, and the vessels are so small, but The Ottawa Hospital does more of these intricate procedures than any other hospital in Ontario.”
— Dr. Sudhir Nagpal
“Even though I was getting treated for my leg ulcers, they didn’t improve in size or seem to get any better. And they were painful too,” says Mina, an 89 year old retired music teacher and lifelong musician.
Mina with her husband, Stan.
Mina’s ulcers were caused by atherosclerosis, a condition where an artery’s blood circulation is slowed because of plaque buildup. While the condition is commonly caused by diabetes, it can also develop with age. Without medical attention, the ulcers can worsen, causing infections or risk of losing a limb.
“If Mina’s leg ulcers worsened, we would have to amputate her legs to save her life,” says Dr. Sudhir Nagpal, division chief of vascular surgery at The Ottawa Hospital and surgeon in Mina’s care. While it would save her life, a double amputation would mean Mina could no longer use the foot pedals of her piano — which she plays every day. “It’s been the strength of my life to be able to play the piano,” says Mina. “I knew something would have to be done.”
After a CT scan in 2020 revealed blood clots had formed in both of Mina’s legs, her care team decided it was time to take action.
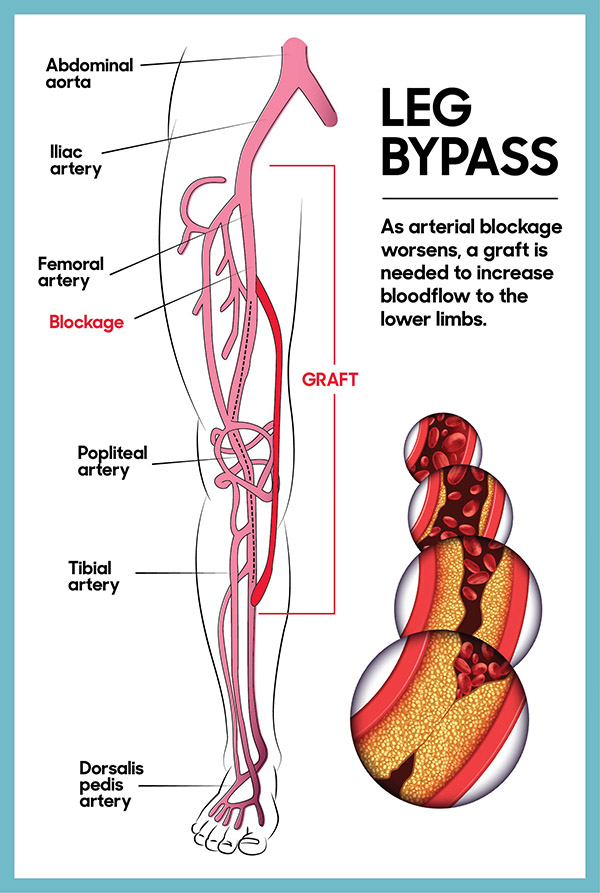
Bypassing the blockage
Leg bypass illustration: as arterial blockage worsens, a graft is needed to increase bloodflow to the lower limbs.
Luckily, Mina’s ulcers hadn’t progressed to the point where she needed full amputations and surgery was still a viable option.
In August 2020, surgeons and interventional radiologists at our hospital were able to perform a minimally invasive surgery on her right leg, placing a stent in the artery, to improve blood flow and keep the artery open. However, this approach didn’t work for her other leg.
To get blood flowing in her left leg, surgeons performed a complex leg artery bypass surgery, rerouting her blood supply around the blocked artery with a graft – like a road detour. During Mina’s nearly five hour procedure, a team of highly-skilled experts in vascular surgery used magnifying glasses to carefully connect Mina’s vein around the blocked artery, above and below the obstruction, to create a new route for blood to flow.
Thankfully, Mina had access to this specialized surgical technique at our hospital — a procedure not available everywhere.
“Bypass surgeries are very complex and take several hours to complete. Not every hospital is able to perform these surgeries because they’re so technically demanding, and the vessels are so small, but The Ottawa Hospital does more of these intricate procedures than any other hospital in Ontario,” says Dr. Nagpal.
Identifying a safer anesthesia option – thanks to research
At the time of Mina’s surgery, our researchers had just wrapped up a study on anesthesia and leg artery bypass surgery. The study, which was published in The British Medical Journal in November 2020, showed that patients who had surgery to improve blood flow in their legs fared better and were able to leave the hospital earlier if they had lighter forms of anesthesia, such as epidural anesthesia, that don’t require a breathing tube.
Dr. Sudhir Nagpal, division chief of vascular surgery at The Ottawa Hospital.
“We’re able to provide excellent, nation-leading clinical care because of the experts we have access to and the research happening right here in the clinic at The Ottawa Hospital.”
— Dr. Sudhir Nagpal
Because Mina’s surgeons had early access to the study’s results at the time of her procedure, they were able to recommend that she opt for the epidural anesthesia. “They asked me what kind of anesthesia I wanted to have and described the different ones but suggested that being 89, it would be safer to get the epidural,” says Mina. “And it all went really smoothly.”
According to Dr. Nagpal, having this research happening under our roof is critical. “Mina was able to benefit from some of the research we’re doing and have a better outcome.”
Access to world-class care
Despite the complexity, Mina’s surgeries were a success. But her path back to the piano wasn’t over yet. One week after her surgery, Mina was discharged to continue her recovery at home with the help of virtual care through the LPC.
The clinic, which began as a pilot project several years ago, brings together care providers from across our hospital with expertise in lower-body wounds. While in the clinic’s care, patients like Mina have access to experts in vascular surgery, wound care, plastic surgery, infection prevention and control, orthopedics, chiropody, and more. The model of care means that patients can access the experts they need without long delays. In fact, it’s a model that hospitals across the country are looking to follow.
“The collaboration between multiple different skill sets and specialties all in one place is what really separates our Limb Preservation Clinic from others like it in Canada,” explains Dr. Nagpal. “We’re able to provide excellent, world-class clinical care because of the experts we have access to and the research happening right here in the clinic at The Ottawa Hospital.”
Mina with son David, daughter Jennifer, and husband Stan.
Mina’s care team tracked the progress of her ulcers through a wound care software called how2trak. With the help of an at-home nurse who made weekly visits to Mina’s home following her surgery, photos of Mina’s leg wounds were uploaded into the software and analyzed by her care team to determine if the wound was getting better or worse over time.
“Through this software, we’re able to see that Mina’s ulcers have gone from being fairly large in size to the point where they’re almost healed,” says Dr. Nagpal. “We can do all this while she’s in the comfort of her home.”
Back at the piano
As Mina’s condition improved, her visits with the at-home nurse and experts in the LPC became less frequent. “I feel quite happy about the way things have gone. I don’t have pain now,” says Mina. “Dr. Nagpal was an excellent doctor.”
“It’s been the strength of my life to be able to play the piano.”
— Mina King
Now, with her ulcers nearly healed and access to the expertise of her care team just a virtual call away, Mina is back to her routine of playing the piano every day — without worry.
“I was very glad to get back home and get back to my piano. I think it was one of the things that helped me recover so quickly,” she says. “When I get tired, or anything’s bothering me, I sit down at the piano and it seems to just take it all away.”
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Patient Care, World-Leading Research
Originally published: May, 2021
Early in the fall of 2020, Michele Juma noticed the vision in her left eye was becoming cloudy. The Sault Ste. Marie resident initially turned to her family doctor for answers. She learned she had a meningioma tumour — and time was not on her side to save her vision. Fearing she would face blindness, Michele, a mom of four, eventually travelled to The Ottawa Hospital where she could receive specialized care — care she could not receive close to home.
It was early November when MRI results revealed the mass at the base of her frontal lobe. “By this time, I lost my ability to see colour in my left eye — my vision was deteriorating. It was like looking through a frosted window,” remembers Michele. While her right eye would start compensating to get her through her day-to-day, Michele was finding the routine of caring for her teenage boys and working a challenge and knew she needed to see a specialist. Soon, she and her husband were making plans for the eight-hour drive to Ottawa to meet with Dr. Danah Albreiki at the University of Ottawa Eye Institute located at The Ottawa Hospital.
Seeking answers at the University of Ottawa Eye Institute
The University of Ottawa Eye Institute was founded in 1992 as the home of The Ottawa Hospital’s Department of Ophthalmology. It is a major clinical, teaching, and research centre in Canada specializing in diseases and conditions that affect the eyes. Dr. Albreiki’s expertise focuses on neuro-ophthalmology and adult strabismus surgery, which focuses on straightening misaligned eyes.
Born and raised in Saudi Arabia, Dr. Albreiki says our Eye Institute plays an international role in sharing our expertise with patients and ophthalmologists in more than 86 countries around the world. As one example, she explains, the Ottawa Eye Institute has an affiliation with India Srikiran Institute of Ophthalmology in Kakinada, Andhra Pradesh. Affiliations like these provide an opportunity for the ophthalmology residents to travel and explore ophthalmology in a very different setting.
Having done her ophthalmology residency in Ottawa, Dr. Albreiki reflects on the importance of teaching. “I think the Eye Institute is honestly an amazing academic place where staff are dedicated first and foremost to their patients, but have a heavy focus for teaching the ophthalmology residents. This ripple effect extends beyond Ottawa and will travel wherever the residents end up working as they share their knowledge and expertise with their communities. As a matter of fact, Michele was seen first by our neuro-ophthalmology fellow Dr. Noran Badeeb who came all the way from Saudi Arabia to train with us.”
Michele with her family.
“The danger is it’s very close to the optic nerve, and Michele is a good example of how people can quickly deteriorate with these tumours, and they are at high risk of losing their vision.”
— Dr. Fahad Alkherayf
By early December, Michele met Dr. Albreiki’s team and she learned what was happening with the tumour. “If we leave tumours that are compressing on the optic nerve for too long, there is a high chance that it will damage the optic nerve which subsequently leads to permanent vision loss,” explains Dr. Albreiki. She adds, “Despite the severe vision loss that had happened, we were able to determine, by way of ophthalmic diagnostic testing, that Michele’s optic nerve appeared more suffocated than actually dead. By removing the suffocation, we would allow the optic nerve to breathe again and there would be a good chance she would regain part, if not all, of her vision.”
For that to happen, they would need to act fast.
Understanding meningioma tumours
Knowing Michele had travelled from Sault Ste. Marie for her initial meeting at the Eye Institute, Dr. Albreiki arranged for her to meet later that day with world-class, skull base surgeon Dr. Fahad Alkherayf who set in motion a plan to remove the mass.
He explained to Michele that she had a skull base meningioma. The tumour was about three centimetres by three centimetres — about the size of a golf ball. The biggest challenge with removing these types of tumours is often their location. “How you can reach it without damaging the brain around it and the things attached to it is key. If you’re not careful, and you end up injuring any of these structures, unfortunately, the outcome is devastating,” explains Dr. Alkherayf.
“The Ottawa Hospital is one of the main leading centres in minimally invasive skull base surgery, and I think that speaks to the expertise we have in our centre.”
— Dr. Fahad Alkherayf
Minimally invasive surgery offers new treatment options
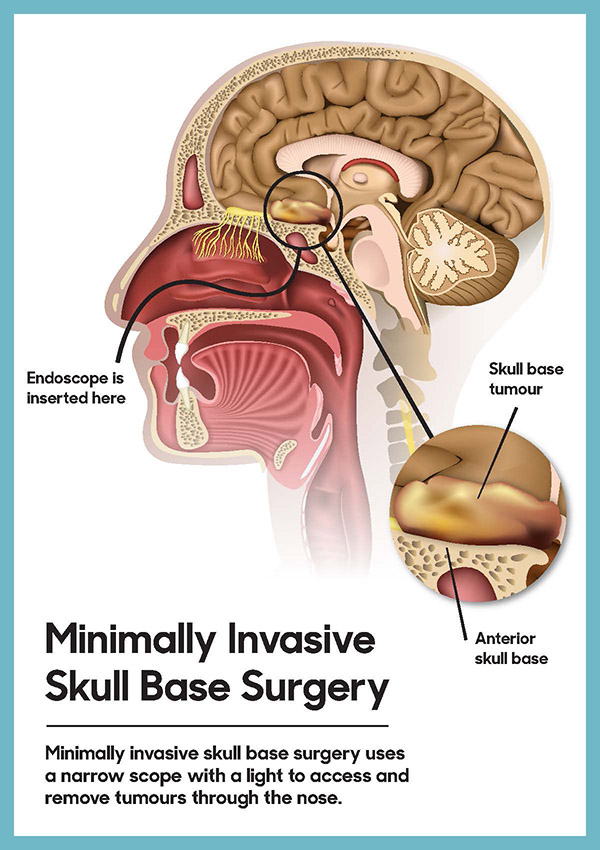
Minimally invasive skull base surgery uses a narrow scope with a light to access and remove tumours through the nose.
The treatment used today for a meningioma tumour is relatively new. In the past, it was a much more invasive procedure known as a craniotomy, which results in a large incision with a higher risk of injuring the optic nerve. However, today minimally invasive surgery allows much more effective and safer care for our patients. “Instead of the old, traditional way of going through the skull, and lifting the brain — today, we go through the nose,” explains Dr. Alkherayf. This means no incision, faster recovery time, reduced pain, a higher accuracy rate compared to traditional open surgery, and a shorter hospital stay.
The Ottawa Hospital has established itself as a leader in Canada when it comes to this type of minimally invasive surgery. Dr. Alkherayf says we’re one of the largest centres in Canada doing it. “If we look across the country, The Ottawa Hospital is one of the main leading centres in minimally invasive skull base surgery, and I think that speaks to the expertise we have in our centre. It’s not just surgeons but it takes a good anesthesia, nursing, and neurophysiology team, so the surgeon can function well. I think what’s unique about our hospital is we have this full package providing care to our patients.”
Having access to this expertise is a significant advantage for patients like Michele, who required urgent surgery due to the rapid growth of the tumour and the risk of it causing blindness not only in her left eye but in her other eye as well. After meeting with Dr. Alkherayf as well as Dr. Shaun Kilty, an ear, nose, and throat (ENT) specialist, her surgery was scheduled for December 17, 2020.
Michele remembers feeling anxious and nervous. “It was all really overwhelming — and surreal. When I think that I’d been walking around with this tumour probably for years…it was kind of unbelievable to me to think of the whole gravity of the situation.” However, Michele says she knew she was in good hands. “I do have to say that when I met with Drs. Albreiki, Alkherayf, and Kilty, they were very reassuring and answered all our questions, significantly reducing my anxiety.”
Michele being wheeled into surgery at The Ottawa Hospital to remove her meningioma tumour.
Specialized technique used only at The Ottawa Hospital
Leaving their four sons at home, Michele and her husband arrived back in Ottawa just over a week before Christmas. The minimally invasive surgery would last eight hours with Drs. Alkherayf and Kilty working alongside one another to remove the tumour piece by piece — through Michele’s nose.
“The monitoring helped ensure we didn’t pull too hard on her optic nerve. If it wasn’t for this specialized technique, I don’t think we would have achieved the same results.”
— Dr. Fahad Alkherayf
Continuous evoked visual potential goggles are used by surgeons during some brain and skull surgeons to monitor a patient’s vision and avoid damaging the optic nerve.
During the procedure, Dr. Alkherayf was able to monitor Michele’s vision. In fact, our hospital is the only centre in Canada using this specialized technique. “We have established a method where we can receive a signal from the eye, as well as from the optic nerve and the brain, about what’s happening to the vision while the patient is asleep.” Goggles — which resemble swimming goggles — are placed on the patient while they’re under anesthetic. The goggles send a flashing light, which sends a signal into their retina, and then it travels down their optic nerve, crosses the chiasma (the back of the optic nerves where they meet), and then travels to the vision centre of the brain. The signals will change if the surgeon’s pushing or pulling the optic nerves and potentially damaging them.
According to Dr. Alkherayf, this technique was critical during Michele’s surgery. “Her tumour was basically glued to her optic nerve, which explains why she was having this significant vision problem. The monitoring helped ensure we didn’t pull on her optic nerve. If it wasn’t for this specialized technique, I don’t think we might have achieved the same results.”
For the first five days after surgery, Michele says there was a lot of sleeping, but she remembers the moment when she woke up for the first time and she opened her eyes. “My husband was there, and I was able to see — it was right away that I could see again!” Even better news, before Michele was released from the hospital on Christmas Eve, Dr. Alkherayf shared the news she had been hoping for – the tumour was benign, and he was able to completely remove it.
“I’m grateful to be able to watch my sons continue to grow and, of course, to have the chance to be part of the activities they love most, like swimming and hockey.”
— Michele Juma
With this life-changing news in hand, Michele and her husband began their long drive back home to Sault Ste. Marie arriving home at 11:30 p.m. on December 24, just in time to be with their children for Christmas. “It was like a Hallmark movie,” laughs Michele.
Michele, with her husband and four sons, after arriving home in time for Christmas in 2020.
Today, her vision is fully restored. She’s back at work and keeping up with the busy life that comes with raising four teenage boys. “I consider myself to be so incredibly fortunate to have had Drs. Alkherayf and Kilty conduct this surgery. When I think about the complexity of what they did, I never cease to be amazed, and I feel truly blessed.”
While she and her family truly appreciate the exceptional skill of both physicians, Michele adds they were kind, compassionate, and empathic throughout her journey. “As scary as all this was, I can honestly say that I always felt confident that I was in very good hands.” She adds, “I’m grateful to be able to watch my sons continue to grow and, of course, to have the chance to be part of the activities they love most, like swimming and hockey.”
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: COVID-19, Innovation and Technology, Patient Care, Technology
When COVID-19 moved into the Ottawa region in March of 2020, we were in uncharted territory. However, despite the rapidly changing information in the early days, and the unknowns about this virus, something very clear began to emerge – unity. The community would soon show an outpouring of support for The Ottawa Hospital while healthcare teams rallied together to care for patients.
“Thank you to our generous donors – some who reached out for the first time.” – Tim Kluke
As our front-line workers would go into the hospital each day to face the virus head-on, the community stayed home to help flatten the curve. Nevertheless, it became obvious residents wanted to do more – and they did. Donations both big and small began streaming in and the COVID-19 Emergency Response Fund was created. To date, more than $2 million has been generously donated to support our hospital’s COVID-19 efforts and these donations have already been put to work. Tim Kluke, President and CEO of The Ottawa Hospital Foundation, says this support has made a world of a difference supporting both research and care projects. “This proves once again that we really are stronger when we pull together. Thank you to our generous donors – some of whom have even reached out for the first time. Research currently underway will allow us to better understand and treat the virus, to keep our patients and our community safe.” Donations continue to be accepted today.
Personal Protective Equipment (PPE) was another way our community lent a helping hand. The Ottawa Chinese Community quickly mobilized and raised over $120,000 to purchase necessary equipment like ventilators and PPE for our staff.
In Their Own Words: Good Days, Bad Days, and What Keeps Them Coming Back
Stepping into the unknown
While the community united to show their support for our front-line workers, a COVID-19 floor was created at both the General and Civic Campuses to care for the patients who tested positive for the virus. The team at the General Campus that had originally cared for Thoracic, ENT (Ear, Nose, and Throat), and surgical patients would, almost overnight, become the team caring for COVID-19 patients. Little did they know at the time, they would be caring for these patients for well over a year. “We have a background in lungs and breathing issues on our unit, so we were a natural fit to care for these patients,” says Vanessa Large, a registered nurse at our hospital for the past four years.
Vanessa Large, Kristine Belmore, and Leah Mills worked on the “COVID floor” in 2020. Pictured above wearing personal protective equipment (Image 1) and without (Image 2).
Nevertheless, it was a daunting and draining task. Kristine Belmore is a registered nurse who has been at our hospital for 11 years and never did she imagine her career taking this step. “I was working the day the first positive patients came in. We were constantly getting new updates on protocols for caring for these patients – not just daily but during our shifts,” says Belmore. She adds, “It was the equivalent of how I felt when I was a new nurse preparing for a shift — I didn’t sleep well. I was anxious and there was the fear of the unknown.”
Leah Mills was just three years into her career as a registered nurse when she found herself caring for COVID-19 patients. “There was no easing into the COVID transition; it turned our world upside down,” says Leah.
Resilience as weeks turn into months
Dr. Samantha Halman helps a patient communicate with their loved ones via an iPad.
In those early weeks of caring for patients, there was the struggle of watching some patients go from appearing stable to suddenly clinging to life. Those days would take an emotional toll on these nurses. “The increase in demand during the surge of patients was overwhelming. Over time it became easier because we had concrete policies in place and we started recognizing a pattern in patient’s decline,” recalls Leah.
“We became their only sources of human connection, we became their second family. We would be there holding an iPad so they could see the friendly smile of a loved one – sometimes it was to say goodbye.” – Vanessa Large
The playbook had to be reinvented and new ideas had to be considered to help calm patients when they struggled to breathe or feared what might happen next. Then there were the layers of PPE, which created an additional level of safety but also a new challenge. “Caring for patients, especially the elderly who can be confused, was difficult because they can’t see your facial expressions – we had to find new ways to reassure patients when they were scared. We also became the link between the patient and the family, through phone calls and video calls – something we’ve never done before,” says Kristine.
Vanessa agrees adding, “We became their only sources of human connection, we became their second family. We would be there holding an iPad so they could see the friendly smile of a loved one – sometimes it was to say goodbye.”
Mentally and emotionally, the long haul of this pandemic started to wear on these nurses. Leah explains they’re used to helping patients heal and get better. “We’re feeling burned out and exhausted seeing patients decline quickly and sometimes die. It’s not what I’ve been used to in my role.”
Thankfully, over the past year, this dedicated care team has helped ensure the majority of COVID-19 patients have been able to regain their health and return home to their loved ones.
The nurses of the “COVID floor”
“Working on the COVID-19 Unit, with the numbers going up and down, you never know which point is going to be the tipping point.” — Leah
“The best part about starting on the COVID-19 Unit was the team. Everyone was very supportive, willing to teach the newbies on the unit. And, the patients especially, they were very accommodating, and I will remember them for a long time to come.” — Margaret
“My worst part of this year was seeing a lot of suffering and not being able to help as much as I would want to.” — Michael
“COVID-19 has taught me to really value and cherish the time that I had with my family, my friends, and my colleagues.” — Jeannette
COVID-19 patient grateful for compassionate care
One of the patients, who experienced firsthand compassionate care on the COVID-19 floor, was Fr. Alex Michalopulos. The Greek Orthodox priest spent 10 days in our hospital. He couldn’t be more thankful to be feeling better today. “For the times when the doctors or nurses came in to see me, for the times when I was reassured—I’m thankful I was well taken care of with love and respect for human life.”
“I have a lot more respect for the medical professionals. I always had, but this time it was at a different level. They were there for me.” – Fr. Alex Michalopulos
Father Alex Michalopoulos of the Greek Orthodox Church. Father Alex was treated for COVID-19 at The Ottawa Hospital last year.
As tears well up in his eyes, and he stops briefly to regain his emotions, Fr. Michalopulos says it’s sometimes good to be on the other side, to feel what others are going through. “I have a lot more respect for the medical professionals. I always had, but this time it was at a different level. They were there for me.”
He adds, “They held my hand. They showed compassion. They showed a lot of respect and love. I will be forever grateful for them.” It was that special touch, and care from complete strangers that helped give Fr. Michalopulos the strength to get back home to the family he loves and eventually to his parish family.
“I will always remember how I was treated by strangers. I admire them and will always pray for them.”
In an effort to do his part to help, Fr. Michalopulos is participating in research that is investigating the long-term effects of the virus. Drs. Sara J. Abdallah and Juthaporn Cowan are checking in on participating patients, like Fr. Michalopulos at three, six, and 12 months after they were initially infected.
He explains why it was important to become involved. “I thought it would be useful to help researchers understand the effects and lingering effects of the virus in gathering information to help create a vaccine and or a cure.”
Giving back through research
Researchers at our hospital have been deeply involved in the global race to combat COVID-19. They are exploring more than 60 research projects to support the worldwide effort to find better ways to treat and prevent the virus. A number of those projects have been supported by donors through the COVID-19 Emergency Response Fund, including a world-first clinical trial, led by Dr. Rebecca Auer, which aims to protect cancer patients from COVID-19 – to date, 22 patients, have been recruited.
Dr. John Bell is a senior scientist in the cancer therapeutics program at The Ottawa Hospital.
Dr. Carolina Ilkow is a scientist in the cancer therapeutics program at The Ottawa Hospital.
Drs. John Bell and Carolina Ilkow are harnessing their expertise in making cancer-fighting viruses to develop a vaccine against COVID-19 — a made-in-Canada solution. In addition, our Biotherapeutics Manufacturing Centre is helping to manufacture three other COVID vaccines for clinical trials, as well as an experimental stem cell therapy.
Pushing forward despite a challenging year
As research continues to produce more answers and vaccines continue to roll out across the region, the team caring for patients remains steadfast. “The vaccine brings us hope. I remember how exciting it was when I received mine,” says Kristine.
Venus Lucero, a nurse at The Ottawa Hospital, administers the hospital’s first dose of the COVID vaccine.
There is hope someday they can start getting back to the way things used to be, or at least close to it. For Kristine, it would mean not worrying about hugging her children when she comes home from work.
For Leah, it would mean letting her mind shut off for the first time in a year – and truly relax. For Vanessa, it would mean the excitement of spending time with her fiancé, Colin – also a frontline worker – as they’ve been isolated from each other during the pandemic. Despite the challenges, each one takes great pride in the care they’ve been able to provide during these unprecedented times. And how they also helped each other along the way.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Biotherapeutics, COVID-19, Donors, Gratitude Award, Patient Care, World-Leading Research
Amidst exciting new updates from research projects supported in earlier rounds of funding from the COVID-19 Emergency Respond Fund, two new projects are now getting underway. Thanks to donor support from our generous community, more than 50 research and innovation projects are in progress and are helping us better understand and address COVID-19.
COVID-19 and rheumatoid arthritis: using big data to understand risks and improve treatments
Dr. Sibel Aydin
With more than 30 million infections worldwide, researchers now have access to massive amounts of data to try to understand why COVID-19 causes severe illness in some people and mild or no symptoms in others. Factors like age, hypertension and obesity clearly play a role, and it is possible that certain immune disorders may also have an impact. Dr. Sibel Aydin is using a big data approach to determine if people with the immune disorder rheumatoid arthritis are more or less likely to get severely ill with COVID-19. Harnessing data from ICES and the Ontario Best Practice Research Initiative, her team will also look at the impact of immune-suppressing drugs that are commonly used to treat rheumatoid arthritis. This research could improve our global understanding of COVID-19 and lead to better treatments for people with both COVID-19 and rheumatoid arthritis.
Understanding the impact of COVID-19 on women
Dr. Innie Chen
Dr. Innie Chen is leading research to understand the impact of COVID-19 on women, thanks to seed funding through the COVID-19 Emergency Response Fund.
COVID-19 is affecting women in many ways, from increased caregiving responsibilities to increased risks of domestic violence. Women are also more likely to work in healthcare jobs that have a higher risk of exposure to COVID-19. Finally, women may be negatively affected by delays in access to health care associated with COVID-19.
Dr. Chen has assembled an internationally recognized team that will help understand and address this challenge by developing core outcomes for women’s health equity during Covid-19. The researchers will perform a systematic search of the literature and assemble a multidisciplinary panel of community patient partners and healthcare workers to identify the key issues in women’s health during the pandemic. This information will lead to evidence-based strategies to mitigate gender-based impacts and help improve the lives of women during the pandemic.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: COVID-19, World-Leading Research
It was a routine patrol in Kandahar that altered the course of Bushra Saeed-Khan’s life forever. In one brief instant, the detonation of an improvised explosive device (IED) changed everything. She went from a Federal employee on an assignment in Afghanistan, to an amputee trauma survivor grappling with Post-Traumatic Stress Disorder (PTSD). The complexity of Bushra’s traumatic injuries brought her to The Ottawa Hospital where a dedicated team of experts were ready to help her get back home.
Facing a war zone
Bushra was just eight weeks into a year-long tour in Afghanistan when she received permission to accompany troops “outside of the wire” – beyond the protection and confines of a military base. When their mission was complete, they headed back. It was then the light armoured vehicle (LAV) Bushra was travelling in ran over an IED buried underground.
Bushra (left), in Kandahar, prior to departing the base on the day of the attack.
She recalls hearing a loud bang, one unlike anything she’s ever heard, before being momentarily knocked out. When she came to, there was silence. Confusion and shock paralyzed her entire body. But it didn’t matter; she was pinned down inside the vehicle, unable to move. Fear filled her every thought. Was she the only survivor? Could the vehicle go up in flames while she was stuck inside it? Was there anyone around to save her? Each racing thought was as anxiety-inducing as the other, while in a war-torn country, miles away from base, from safety, her family, and her home.
Four soldiers and one civilian, who had become Bushra’s friend, died that day, on December 30, 2009. Bushra, one of just five survivors, is lucky to be alive. But she didn’t walk away unscathed. To this day, she continues to feel the ripple effects of the incident more than a decade later.
Seeking medical attention
After witnessing the explosion, troops in the second LAV acted quickly, requesting back up to assist the survivors. As they came to Bushra’s aid, it was clear her injuries were severe. Her entire body was affected by the blast. The force of the explosion was so fierce it left Bushra’s abdomen exposed, and her legs critically wounded – a portion of one completely gone.
Bushra waking in Germany.
Bushra was airlifted by helicopter to a military base for emergency medical care before she was transported to a hospital in Landstuhl, Germany, where she was placed in a medically induced coma. As doctors worked to stabilize her for the long flight to the Trauma Centre at The Ottawa Hospital’s Civic Campus, Bushra was introduced to the name Dr. Nancy Dudek, Medical Director of the Amputee Program. Bushra needed to start to think about recovery and Dr. Dudek would soon become Bushra’s primary caregiver for over a decade. “I didn’t realize at the time just how much of an impact Dr. Dudek would have on my life.”
Road to healing and recovery
Once Bushra was in our care, experts began working around the clock to repair the extensive damage that had been done by the IED. “I remember the first time I met Bushra,” says Dr. Dudek. “She had just arrived at the hospital and had a lot of injuries. The most critical question I had for her at that time was regarding her leg.” Bushra’s leg was severely damaged, and it was clear they would have to amputate it. Since her femur bone was also fractured, they needed to decide if her orthopedic surgeon would perform a full amputation of the leg or fix her femur and save as much of her leg as possible. “It’s really important, when possible, to include the person who will be receiving the amputation in that decision,” says Dr. Dudek. “We want our patients to have a say in what’s going to happen to their body.” In the end, as a team, they decided to fix Bushra’s fractured femur and perform a through-knee amputation.
This was the first of several surgeries Bushra underwent at our hospital. “Within the first week of being in the trauma unit I had what felt like over 20 surgeries,” says Bushra. “That’s when I stopped trying to keep track.”
The women of the Rehab Centre
Once Bushra was medically well enough to leave the trauma unit, she was moved to the Rehabilitation Centre. This is where she would remain for over a year as an inpatient, followed by six months as an outpatient. Under the care of some of the best physiotherapists and prosthetists in the field, Bushra had to relearn how to perform the most basic tasks, such as lifting her arms, moving her head and sitting upright in bed, before eventually learning how to walk with a prosthetic leg. “I call them ‘the women of the Rehab Centre,’” says Bushra. “They’re just so brilliant in their respective fields, but also so kind and caring. It was really nice to see.”
Bushra learning to stand again.
At the time, Bushra was still in great discomfort, not just from her surgeries but from flashbacks of the incident, her survivor’s guilt, and the thought of living the rest of her life with a disability. Working through those emotions felt like mountains she had to climb and conquer, and some days they were too much to bear. “At one point, I even contemplated suicide. Some days I couldn’t even get out of bed. Not just because of the physical reasons, but mentally I couldn’t deal with everything I had to fight through that day,” says Bushra. It wasn’t long before she was introduced to Dr. Josie Marino, a now-retired psychologist at our hospital. Dr. Marino was instrumental in Bushra’s care, helping her overcome those mental obstacles. “PTSD never really goes away, it comes back when times get rough, but Josie gave me the tools that I needed to cope,” Bushra explains.
“I like giving patients the confidence that they can do more than they think,” – Marie Andrée.
On those more difficult days, Bushra’s physiotherapist, Marie Andrée Paquin, would adapt and cater the exercises to the pain she was experiencing. If Bushra didn’t feel well enough to leave her room, Marie Andrée would have her perform exercises in bed. On the days she was feeling stronger, she would push her a little bit further. “I like giving patients the confidence that they can do more than they think,” says Marie Andrée.
She even went as far as having Bushra perform exercises that mimicked dance moves so that she could dance at her sister’s wedding. “It was really nice that they were so flexible in my care, tailoring it to exactly what I needed,” says Bushra.
Discovering hope
Bushra’s prosthesis.
After Bushra’s amputation, she couldn’t help but worry about the future. After all, she had never met someone with a prosthetic leg. “My family and I were very worried about what type of life I would have,” says Bushra. Realizing this, Dr. Dudek asked a former patient of hers to visit with Bushra. “I remember so clearly, this woman walking into my trauma unit room. It was shocking for me to see her walking around and playing with her kids,” says Bushra. “I am thankful that Dr. Dudek introduced me to this woman. That was a pivotal moment for me.” After that meeting, Bushra no longer worried. Rather, she was filled with hope.
This gave Bushra the confidence she needed to try a prosthetic leg. She met with Laura Scholtes, a prosthetist at our hospital, who fitted her with a new artificial limb. It wasn’t long before she got the hang of it and once she did, she was introduced to the Computer-Assisted Rehabilitation Environment (CAREN) System.
The CAREN System
Bushra hasn’t been the only patient who has experienced injury in Afghanistan. In realizing the need, the Canadian Armed Forces and our community raised funds to bring this virtual reality system to Ottawa — one of only two cities in Canada who have it. The CAREN System has been instrumental for patients in the Rehab Centre.
Bushra on the CAREN System.
“The CAREN System was amazing,” says Bushra, when asked about her experience with this unique virtual reality rehabilitation equipment. It combines incredibly large 3D graphics and a platform that moves with the person as they explore a virtual 3D world on a remote-controlled treadmill. “It’s very safe and a great way to challenge a patient’s balance,” explains Marie Andrée.
“The CAREN System was really a catalyst in my recovery as I was able to learn how to walk with a prosthesis and push myself in an environment that I knew was safe,” says Bushra. “And it trains you to walk on all kinds of surfaces. There was even a setting for paddle boarding. It was really a lot of fun.” Training in the CAREN System boosted her confidence. Today she’s riding her bicycle, and excelling in her career as a diplomat, something she didn’t expect she would be able to do.
New life after trauma
Bushra holding her daughter.
One of the very first questions on Bushra’s mind after her surgery to reconstruct her abdomen was whether or not she would be able to have a baby. The injuries were so extensive that surgeons had to insert a mesh lining to help rebuild the abdominal wall. At the time, her physicians were unsure if her body would be able to adapt to carry a child to full term. Eight years later, Bushra announced she was pregnant, and much like she adapted to a new normal with a disability, her body was able to adapt to a growing baby.
“They are my guardian angels. My heroes. They saved my life.” – Bushra Saeed-Khan
As Bushra’s belly grew, so did her challenges with her prosthesis. Laura was able to monitor Bushra throughout the duration of her pregnancy to ensure that her prosthesis fit her limb comfortably. But in the last two months of her pregnancy, Bushra was no longer able to walk with ease and temporarily switched to a wheelchair. As she was prepped to undergo a c-section, Dr. Dudek worked alongside Bushra’s obstetrician, Dr. Laura M. Gaudet, to ensure that Bushra had the most accessible birthing room possible, one with a doorframe wide enough to fit her wheelchair, and a bed that could be lowered so that she could more easily get in and out.
The day after Bushra gave birth to a beautiful baby girl, Dr. Dudek was there to meet her. “After my initial surgery, my doctors weren’t sure if I would be able to have children. And then eight years later there was Dr. Dudek holding my baby,” says Bushra. “So, it was a special moment. It really felt like everything was coming full circle.”
Today, Bushra is able to play with her two-year-old daughter, just like the patient she met in hospital with the prosthetic leg early on in her recovery. Those feelings of hope have become reality.
More than a decade later
More than a decade after the incident, it would be easy to look at Bushra and be impressed by how far she’s come. But she accepts each compliment about her recovery with humility, because she knows she didn’t do it alone – she was backed by some of the best healthcare workers in the country. “I’m a product of my circumstances and I was fortunate to have the support structure offered by the Rehab Centre at The Ottawa Hospital,” says Bushra. “It felt like a team effort and it’s thanks to my caregivers that I was able to gain independence. They are my guardian angels. My heroes. They saved my life.”
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Creating Tomorrow, Patient Care, Rehab, Technology, Trauma
The study that is changing breast cancer treatment around the world
There is such deep love in Gina Mertikas-Lavictoire’s eyes when she looks at her three young children. But there is something else, too: fear. Fear that one or even both of her daughters will develop the same aggressive breast cancer she’s had. So, when an opportunity arose to participate in a clinical trial through The Ottawa Hospital’s REthinking Clinical Trials (REaCT) program, she readily agreed.
Gina and family
“I’m really big on clinical trials,” says Gina, “so I had no hesitation helping…and I trusted Dr. Clemons.”
Dr. Mark Clemons, scientist and oncologist at The Ottawa Hospital, was Gina’s medical oncologist and also the one who launched REaCT in 2014, together with Dr. Dean Fergusson, senior scientist and Director of The Ottawa Hospital’s Clinical Epidemiology Program, and others. The purpose of REaCT was to make enrollment in clinical trials easier for cancer patients. The more patients who enroll, the more that can be learned, which leads to better treatments and practices.
“When you think the most common killer is now cancer,” says Dr. Clemons, “and only 3% of patients are involved in trials, it’s quite shocking. Patients are desperate to help, not just for themselves but for their children. They want their children to have better treatments if this happens to them.”
Study focused on safer care, less cost, fewer hospital visits
Gina participated in a study focused on a drug called filgrastim, which boosts the production of infection-fighting white blood cells. People with early-stage breast cancer often receive daily injections of the drug at the start of every cycle of chemotherapy, anywhere from five doses to seven to 10. Many cancer patients struggle with both the cost of the drugs, at more than $200 per injection, and the side effects.
“This is an incredibly expensive drug,” says Dr. Clemons, “but often patients feel horrible with it. It makes you feel miserable.”
Up to this point, there had been conflicting debate on how many injections worked best. So, after reviewing all the evidence and surveying doctors and patients, Dr. Clemons and his colleagues launched a clinical trial to find out, enrolling 466 patients from seven Canadian cancer centres.
Gina was among those patients, giving herself a daily shot of filgrastim 10 days in a row after each of her three rounds of chemotherapy.
Gina presenting a cheque to Dr. Clemons in support of the REaCT program at The Ottawa Hospital
“I’m so thankful I was part of this trial”
Gina says she had no hesitation volunteering to be part of this trial, “because I’m able to help future breast cancer patients,” adding, “We are helping the future generation with every trial we do, so I’m happy they asked me.”
She’s happy, too, with the results of the study, published in Annals of Oncology, which have helped change care globally. Researchers discovered that five doses of filgrastim are just as good as seven to 10 doses in terms of preventing infections. And when they looked at treatment-related hospitalizations, they found that five doses are better: patients who received five doses had a 3.3 percent chance of hospitalization for side-effects compared to 10.9 percent for people who had seven to 10 doses, a difference of more than three-fold.
“I believe this is how we will find the cure for cancer.”
– Gina Mertikas-Lavictoire
Results change global standard of care
Drs. Mark Clemons and Dean Fergusson developed the Rethinking Clinical Trials or REaCT program
“This study is already changing practice around the world,” says Dr. Clemons. “It is making our patients healthier and giving them more time with loved ones by reducing unnecessary hospital visits. It is also saving our healthcare system millions of dollars every year.”
“This study is already changing practice around the world. It is making our patients healthier and giving them more time with loved ones.”
– Dr. Mark Clemons
The REaCT team wants to take this research one step further to find out whether even fewer doses can be prescribed. They have just applied for funding to start that study and are focused on several other clinical trials as well. With more than 2,700 patients participating in 17 trials in 15 centres across Canada, REaCT is now the largest cancer clinical trials program of its kind in the country.
“By thinking differently and using innovative approaches, we are efficiently answering some of the most important questions for patients and for our healthcare system,” says Dr. Fergusson. “The Ottawa Hospital is a leader in this kind of innovative research and our patients are among the first to benefit.”
Gina knows that well. She’s participated in two other clinical trials through REaCT and has become an ardent fundraiser, securing more than $25,000 for cancer research at The Ottawa Hospital.
“I believe this is how we will find the cure for cancer,” she says, “so we really need to continue to support this avenue, to support the next generation of cancer patients.”
“The Ottawa Hospital is a leader in this kind of innovative research and our patients are among the first to benefit.”
— Dr. Dean Fergusson
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Cancer, Clinical Trials, World-Leading Research
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.