Four new board members bolster the board’s business and medical expertise
Category: Creating Tomorrow
JUNE 24, 2020 OTTAWA, ON – The Ottawa Hospital Foundation welcomed four new members to their Board of Directors in June. Collectively, The Ottawa Hospital Foundation board strives to be the most efficient, effective, and respected hospital foundation in Canada, providing optimal support to The Ottawa Hospital. Each new member strengthens the board with backgrounds in business, finance, and medicine.
The four new board members are:
Russell Jones, prior to his retirement, he was CFO of Shopify Inc. He joined Shopify in early 2011 and took them public in May 2015. Russell also held senior executive roles at Mitel Corporation, Newbridge Networks, Watchfire, and Quake Technologies.
Vanessa Kanu, Chief Financial Officer at Mitel. Vanessa leads Mitel’s global finance operations including accounting, treasury, taxation, planning, and analysis and reporting. She is a 2020 Businesswoman of The Year finalist with the Ottawa Business Women’s Network.
Janet McKeage, Vice-President and Investment Counsellor for RBC PH&N Investment Counsel. Janet provides comprehensive discretionary investment management for high net worth clients, corporations, foundations, and endowment funds throughout Canada and internationally.
Dr. Emily Segal, PhD, CPSych, ExecHealth, Longwood Psychology. Dr. Segal is private clinical psychologist and neuropsychologist in Ottawa who trained at McGill University and Harvard Medical School. She understands the importance of translating the latest advancements in research to clinical use.
Michael Runia, Chair of the Board, welcomed the new board members at a recent virtual meeting. “We’re thrilled to welcome the experience each of these community leaders brings to our board. Their dedication to philanthropy will help steer us forward during these unprecedented times.” The Ottawa Hospital Foundation acknowledged the commitment of three outgoing board members: Sam Bhargava, Susan M.W. Cartwright, and Whitney Fox for their years of service. Members traditionally serve nine-year terms with the board.
About The Ottawa Hospital:
The Ottawa Hospital is one of Canada’s top learning and research hospitals, where excellent care is inspired by research and driven by compassion. As the third-largest employer in Ottawa, our support staff, researchers, nurses, physicians, and volunteers never stop seeking solutions to the most complex healthcare challenges.
Our multi-campus hospital, affiliated with the University of Ottawa, attracts some of the most influential scientific minds from around the world. Our focus on learning and research leads to new techniques and discoveries that are adopted globally to improve patient care.
We are the Regional Trauma Centre for eastern Ontario and have been accredited with Exemplary Standing for healthcare delivery — the highest rating from Accreditation Canada. We are also home to world-leading research programs focused on cancer therapeutics, neuroscience, regenerative medicine, chronic disease, and practice-changing research.
Backed by generous support from the community, we are committed to providing the world-class, compassionate care we would want for our loved ones.
For more information about The Ottawa Hospital, visit ohfoundation.ca.
In the latest round of funding from the COVID-19 Emergency Response Fund, supported entirely through the generosity of donors, new research, innovation, and care projects have been approved for seed funding and will now get underway. These vital projects are the latest initiatives chosen out of more than 160 ideas submitted to the COVID-19 Ideas Hub.
The Hub was created by the hospital to allow any staff, regardless of background or role, to submit innovative ideas to combat COVID-19. Teams of experts evaluated the feasibility, available funding, and whether the idea could positively impact The Ottawa Hospital, patients, and the community.
The following care, innovation, and research projects have been selected for seed funding which is made possible by the many generous donors who supported the COVID-19 Emergency Response Fund – thank you to all who have donated.
Hyperbaric oxygen therapy for COVID pneumonia
Dr. Sylvain Boet
When COVID-19 takes over the lungs, it can feel like you can’t get enough air into your body, no matter how much you gasp. When this kind of COVID pneumonia sets in, the only option is to hook the patient up to an artificial breathing machine (a ventilator), with a tube down the throat (intubation). Unfortunately, only half of people with COVID-19 who require intubation will survive after this invasive, last-resort treatment. Dr. Sylvain Boet and his colleagues believe that hyperbaric oxygen therapy (HBOT) may be able to help some people with COVID-19 pneumonia avoid mechanical ventilation and increase survival. HBOT involves placing patients in a pressurized room or chamber so they can breathe 100% oxygen. It can increase the delivery of oxygen to tissues by 10 to 20-fold and can also boost the immune system and help the body fight infections. Small studies in other countries suggest that HBOT may help treat patients with COVID-19 pneumonia, but more research is needed. Dr. Boet and his team will initiate a study of HBOT in people with COVID-19 pneumonia at The Ottawa Hospital, and will work with colleagues around the world to explore the possibility of expanding the trial to other hospitals.
“Hyperbaric oxygen therapy is safe and non-invasive, and our aim is to help COVID-19 patients with pneumonia avoid the need for an artificial breathing machine.” – Dr. Sylvain Boet, scientist and anesthesiologist at The Ottawa Hospital
UPDATE: Dr. Boet has assembled a team of national and international experts in hyperbaric oxygen therapy and has carried out a systematic review and a media appearance in support of the study. His team has secured approval from Health Canada and Clinical Trials Ontario and recently applied for over $1.2 million in funding for the study. Funding from the COVID-19 Emergency Response Fund provided seed funding for this research project.
Developing innovative solutions to address staff safety is critical during this pandemic. It is vital that our people have the best tools to support them for the duration of the crisis. This initiative will use seed funding to support the development and testing of prototypes for priority Personal Protective Equipment (PPE), devices, and supplies to support patient care and staff safety.
Some of the projects supported by this initiative will look at developing, piloting and evaluating equipment like a helmet-based ventilation system for patients in respiratory distress, 3D printed custom-fit sterilizable masks and glideoscope blades for fast intubation, and producing N100 masks for Operating Room staff. It will also look at evaluating barrier methods such as a negative pressure COVID box to improve the safety of aerosol-generating medical procedures (such as intubation or suction), and at creating virtual reality educational videos for safe practices in clinical settings, including various treatment scenarios and how to safely put on and remove PPE.
Preventing dangerous blood clots in COVID-19 patients
Dr. Lana Castellucci
Drs. Marc Carrier, Lana Castellucci and colleagues are contributing to an international clinical trial to find out whether a high dose of blood thinner can prevent dangerous blood clots in hospitalized COVID-19 patients. About 60 percent of these patients develop blood clots, which can be deadly if they travel to the lungs. Not only can blood thinners prevent clots, there is some evidence that they may also alter the course of a COVID-19 infection by interfering with the ability of the virus to latch onto and invade human cells. Patients hospitalized with COVID-19 already receive a low dose of blood thinner as part of their normal care. The researchers will test whether a higher dose can reduce death, transfer to intensive care or the need for mechanical ventilation. The team will also look at how the treatment affects blood clots and major bleeding. This study will immediately impact the clinical care of patients with severe COVID-19 in 13 sites across Canada as well as at sites in the United States and Europe.
“We know patients with COVID-19 are at higher risk of blood clots, which is why we are looking at ways to protect them,” – Dr. Lana Castellucci, associate scientist at The Ottawa Hospital
UPDATE: The COVID-19 Emergency Fund has helped this team to participate in two blood thinner studies assessing different dosing of blood thinners in COVID-19 patients. To date, 22 patients have been recruited in the ATTACC trial and one in the RAPID COVID COAG trial, which has only recently been open for recruitment.
Leading the way to a common approach for testing strategies in the region
In order to enhance the efficiency of COVID-19 testing, more research is needed to better understand the various testing approaches available and in which settings (e.g. hospital-based or community-based) these testing approaches are most effective.
Currently, a variety of testing approaches are being investigated throughout the region by multiple healthcare groups. Through this project, our hospital will assume a leadership role and create a team that will help to centralize and guide testing strategies adopted across the region.
Having this centralized oversight is especially important to ensuring the safety of healthcare workers, patients, and the public as procedures and surgeries resume.
The team will also develop predictive algorithms for determining the probability of COVID-19 prior to a test being administered and will streamline the use of innovative apps for contact tracing.
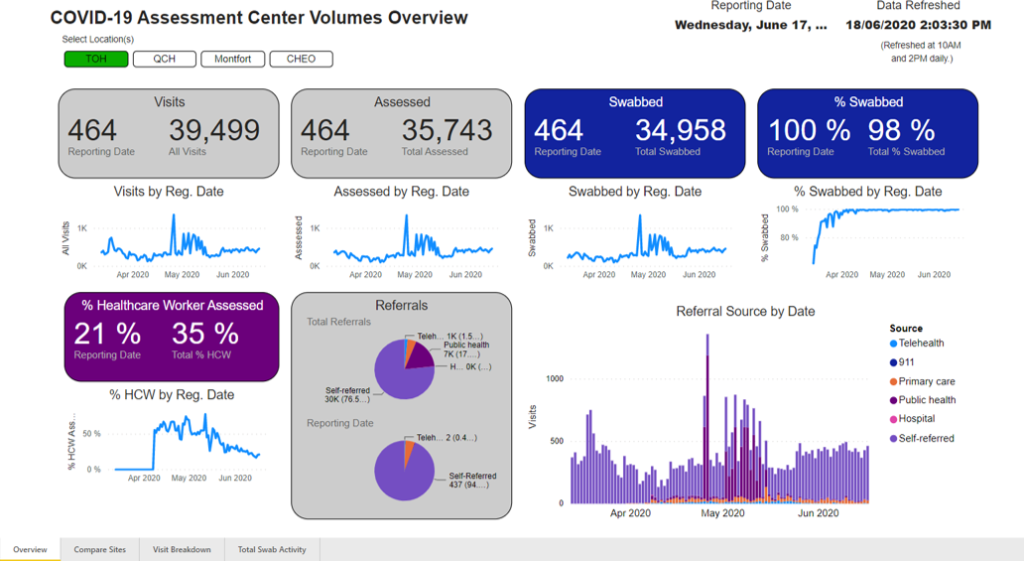
A view of just some of the information a real-time active monitoring system can produce.
Using big data to find promising drugs for COVID-19
Dr. Derek MacFadden
Dr. Derek MacFadden and his colleagues plan to identify promising drugs to treat COVID-19 by analyzing past data from 3,000 Ontario patients treated for other kinds of coronavirus infections between 2014 and 2018. Once the team identifies which drugs are associated with the best patient outcomes, they will use the same process to see how effective those drugs have been at treating patients with COVID-19. The drugs they identify in this screening process would then be tested in a lab to confirm their anti-viral activity against COVID-19. Drugs that pass this stage could potentially be used in future clinical trials for patients infected with or at risk of contracting COVID-19. Unlike most lab-based drug screening approaches, this big data approach has the benefit of seeing how drugs work in humans infected with the virus, and what dose is needed to be effective.
“By looking at which drugs have been successful at treating past coronavirus infections, we can predict which ones are likely to work against COVID-19,” – Dr. Derek MacFadden, scientist at The Ottawa Hospital
UPDATE: Researchers are finalizing their analysis, combing through large amounts of data. Once the analyses are finalized, the research team will be publishing their methods and results. The hope is that these results will be a guide for further research.
To help limit the spread of COVID-19 or any future widespread illness, while also avoiding disruption of care services, it will be essential to explore enhancements of the hospital’s virtual care offerings. With this project, a team will be assembled to evaluate the virtual care initiatives at The Ottawa Hospital.
This initiative will explore topics such as post-discharge virtual care following a surgery, virtual care for populations with chronic illness or disability, adapting ambulatory care to virtual visits, and looking at how virtual options could be used to provide support to our health partners in the community.
Thorough evaluation, including understanding the potential challenges and barriers from the perspective of patients and providers, will be key to determining the feasibility and sustainability of virtual care programs.
Enhancing patient care through data and analytics
Since the beginning of the pandemic, there has been a significant demand for COVID-19 data to support a variety of work at the hospital including research efforts, quality improvement activities, and clinical care. This project will see the creation of a common data mart that leverages the data within Epic, the hospital’s digital health network. This will link data at the individual patient level to COVID-19 infection status, demographics, medical history, lab and medical imaging testing, and pharmacy orders.
This initiative will enable projects using data to look at a variety of topics from evaluating treatment protocols in ICU patients to predicting COVID-19 in certain populations. Ultimately, it will enhance the hospital’s ability to support high-quality patient care and our COVID-19 research agenda.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: COVID-19, Innovation and Technology, World-Leading Research
Now available, in limited quantities, these stunning t-shirts are raising funds for The Craig Kulig Memorial Fund and cancer research at Ottawa Hospital.
We are hoping to send out a small ripple of Wearable Happiness – One t-shirt at a time with all proceeds going to The Craig Kulig Memorial Fund.
Bright and spotted with champagne bubbles that effervesce from the earth, Darlene Kulig’s artworks are utterly joyful. Kulig refers to her style as semi- abstracted spirited landscape. Her stylized art builds on her experience as a graphic designer, and in each new painting she explores light, rhythm, color, and the life force of her subjects. The 12 images in this calendar reflect her home in Canada and her travels abroad.
Darlene’s signature style is described as semi-abstracted spirited landscape and her love of the beauty available in the Canadian landscape is clear. What is especially impressive is that she has developed a unique very personal approach that “feels” Canadian and is utterly joyful.
Darlene’s award winning work has been featured in North American publications and Global Affairs Canada has installed a selection of Kulig Canadian Landscapes in Canadian Embassies buildings around the world. The Mayo clinic has Darlene’s work hanging in the Rochester Clinic and Pomegranate Communications has licensed Darlene’s work in their international product line.
A member of the Etobicoke Art Group and Neilson Park Creative Centre where she studies and paints, you can find her work in galleries across Canada and the United States as well as private collections around the world.
As our researchers move new research projects forward faster than ever in an effort to address COVID-19, donations to the COVID-19 Emergency Response Fund continue to provide seed funding to get these vital projects off the ground. Below are some of the new and promising projects approved for support through the second round of funding. Kick-starting these projects would not have been possible without the support of our generous donors — thank you!
Harnessing cancer-fighting viruses to develop a COVID-19 vaccine
Dr. John Bell
Drs. Carolina Ilkow, John Bell and colleagues are harnessing their expertise in making oncolytic (cancer-fighting) viruses to develop a vaccine against COVID-19, in partnership with scientists and clinicians in Canada and around the world. One of the key things they’ve learned is that the best cancer-killing viruses also stimulate the body’s own immune system – in effect, training the immune cells to recognize and help attack the cancer cells.
They have developed a number of viruses that are very good at boosting the immune system and have already been tested safely in people. These viruses will be reengineered by splicing in key genes from the COVID-19 virus to create several candidate vaccines, which would train the body to mount an immune response against COVID-19. They expect this live vaccine will be particularly important for healthcare workers and vulnerable populations, including people with cancer. Once the vaccine is created, large quantities can be made in The Ottawa Hospital’s Biotherapeutics Manufacturing Centre.
Dr. Carolina Ilkow
“We know that people with cancer who get COVID-19 are much more likely to get severely ill, so we think that working on a vaccine is the best thing we can do right now to help cancer patients.”
– Dr. John Bell
UPDATE: The research team has developed candidate vaccines and laboratory testing is going well. With funding, the team will be ready to do human clinical trials in the new year.
Creating a new mouse model to study COVID-19 lung disease
Dr. Manoj Lalu
Drs. Manoj Lalu, Duncan Stewart and colleagues are working to develop a mouse model of COVID-19 that mimics the severe lung disease seen in humans.
The lack of good, accessible animal models of this disease is severely limiting research around the world. The COVID-19 virus doesn’t infect regular lab mice very well, and the virus is dangerous to work with because it is so contagious for humans.
Drs. Lalu are Stewart are working with Drs. Carolina Ilkow and John Bell, who are creating a novel hybrid virus that features a key protein from the COVID-19 virus (the spike protein) embedded into a well-studied and safe virus called vesicular stomatitis virus (VSV).
The team will test this hybrid virus in mice that have been genetically engineered to be more susceptible to COVID-19, to mimic the severe lung disease seen in humans.
Dr. Duncan Stewart
To make sure the model is accurate, they will use sophisticated techniques to compare their findings in mice with findings from patients, focusing on effects on the lungs, blood and blood vessels. They will then use this model to test new therapies, including mesenchymal stromal cells.
UPDATE: A novel hybrid virus (VSV-Cov2-S) has been manufactured by Dr. Ilkow’s lab with high quality and concentration to proceed with testing in our mouse model. Our experts have worked with the uOttawa Animal Care Committee and have successfully obtained ethics approval. Researchers began challenging ACE2 transgenic mice with the virus in December, controlling for time and dose, and assessing lung injury outcomes.
Studying the immune response of COVID-19 patients in the ICU
Dr. Shirley Mei
Why do some people get severely ill and die of COVID-19, while others experience only mild symptoms? Part of the answer may lie in how an individual’s immune system reacts (and sometimes over-reacts) to the COVID-19 virus. Dr. Shirley Mei and her intensive care research colleagues will study this in critically ill COVID-19 patients using the world’s most advanced “single-cell proteomics” technology.
This technology, called CyTOF, will allow the researchers to study up to 60 different biological factors all at the same time from one single cell. The researchers will create a multi-dimensional map of the immune response to COVID-19, showing how it changes over time and how it sometimes goes out of control.
The data will be shared with clinicians and researchers around the world, in order to improve treatment of COVID-19 and save lives.
UPDATE: Patients participating in this research study will have blood samples taken for a period of 15 days after their enrollment and consent to participate. With approval from the research ethical board, researchers are in the process of recruiting patients into four arms of our study: septic patients in ICU (control cohort), COVID-19 patients in ward (mild disease cohort), ICU patients with severe COVID-19 (severe disease cohort), as well as healthy volunteer (healthy cohort). To date, 34 patients have been recruited with a total of 147 blood samples collected. Pilot experiments to validate the customized immune profiling panel for the mass cytometry (CyTOF) experiment have been completed. This approach will allow researchers to assess the disease progression by using the world’s most advance single-cell proteomics technology.
A balancing act: how to provide regular patient care amid the threat of COVID-19
Dr. Kednapa Thavorn
Dr. Kednapa Thavorn and colleagues will use health administrative data from across Ontario, available through IC/ES, to model the risks of various scenarios for restarting routine clinical procedures in hospitals. Ontario hospitals have postponed many routine clinical procedures in order to preserve resources for COVID-19 patients, but these routine procedures can’t be postponed forever without serious health consequences.
As hospitals contemplate re-staring some routine care, a careful balance will need to be struck between the risks of COVID-19 and the risks of all other preventable diseases and conditions. The model will estimate overall deaths, healthcare costs and other factors for several scenarios, in order to help hospital administrators and policy makers make evidence-based decisions. The model could be adapted for different regions and for different COVID-19 scenarios, including a possible second wave.
UPDATE: Researchers working on this project have developed a detailed protocol of the study and a model structure for a resource optimization model. They have requested the hospital data required for the model and expect to receive this information in January.
Helping COVID-19 survivors stay healthy
Drs. Sara J. Abdallah and Juthaporn Cowan
Drs. Sara J. Abdallah, Juthaporn Cowan and colleagues will study the long-term effects of COVID-19 in survivors, checking in on them three, six and 12 months after they were initially infected. While researchers are beginning to understand what happens in the body during a severe COVID-19 infection, much less is known about the long-term effects in survivors. But based on what is known about other viral infections, the long-term effects could be serious, affecting the lungs, heart and muscles, as well as mental health. Survivors of mild, moderate and severe infections will be included in the study. The researchers will also assess the healthcare resources used by survivors. Results will help improve care for COVID-19 survivors and optimize how healthcare resources are used.
UPDATE: With support from The Ottawa Hospital COVID-19 Emergency Response Fund, researchers set out to understand the medium and long-term impact of COVID-19 on overall health. As of October 31, 2020, 64 enrolled participants completed comprehensive cardiopulmonary testing and important progress has been made in understanding the residual effects of COVID-19 on heart and lung function. As patients continue to be monitored at six and 12-months after COVID-19 infection, our researchers hope that their findings will inform future management strategies for post-COVID breathlessness.
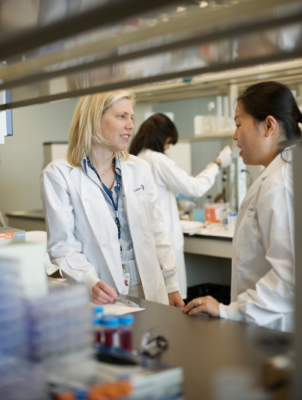
World-first clinical trial aims to protect cancer patients from COVID-19
Dr. Rebecca Auer speaks with a colleague (Photo taken before COVID-19)
Surgeon-scientist Dr. Rebecca Auer is leading a world-first clinical trial that she hopes will protect cancer patients from COVID-19 and other respiratory infections by boosting their immune systems during treatment.
In collaboration with scientists at the Ontario Institute of Cancer Research, researchers will explore an immune-stimulator called IMM-101. The trial will be designed and run by the Canadian Cancer Trials Group at Queen’s University at nine cancer centres across Canada and will recruit 1,500 patients currently receiving cancer treatment.
This trial takes advantage of a lesser-known aspect of the immune system — innate immunity. This first-response arm of the immune system plays a key role in detecting viruses. The research team hopes the IMM-101 treatment will train the patient’s innate immune system to fight off the COVID-19 virus, in addition to other viruses that cause respiratory infections.
The advantage of this immune-boosting approach is that it could help cancer patients fight off all sorts of viruses while they are undergoing cancer treatments and are at their most vulnerable.
The trial has been approved by Health Canada and will run this summer and into the fall. Researchers expect to see preliminary results in about nine months.
UPDATE: The clinical trial was activated in September and is now open in Ottawa for recruitment. The trial will enroll 1,500 patients across Canada, with approximately 200 patients from Ottawa. These Ottawa patients will be part of the translational study funded in part by the COVID-19 Emergency Response Fund.
“While there are many specific vaccines for COVID-19 in the works, they won’t be available for at least a year. Cancer patients need protection now.”
– Dr. Rebecca Auer
The COVID-19 research taking place at The Ottawa Hospital has the potential to transform our understanding of this virus and lead to new ways to prevent and treat it and save lives. This vital research is possible thanks to support from the community. Please consider giving today in support of the COVID-19 Emergency Response Fund.
To find out more about our COVID-19 research and the many collaborators working to make these projects happen, please visit The Ottawa Hospital’s Research Institute.
Keep checking back for more updates on how donations are being put to work right away and are making a difference in The Ottawa Hospital’s fight against COVID-19. To get regular updates sent directly to your inbox, sign up for our newsletter, Vital Links.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Biotherapeutics, COVID-19, World-Leading Research
Solutions to some of our greatest healthcare challenges in the midst of the ever-changing COVID-19 pandemic, won’t come from one idea or one person. Innovation will come from a community of researchers, and academics, and also from front-line healthcare workers, support staff, volunteers and patients. To capture ideas for COVID-19 research and patient care innovations, The Ottawa Hospital responded quickly after the pandemic hit and launched the Ideas Hub, and it’s open to anyone at the hospital who has an idea to contribute— big or small. It is in large part thanks to donor support that we can accelerate the implementation of some of these creative ideas across our hospital.
Once ideas are submitted, within days they are triaged to expert teams assigned to evaluate the feasibility and potential impact of each. Coupled with the overwhelming support of our community, many will receive funding, and in turn, spark innovation at our hospital to help keep staff and patients safe as we continue to navigate the COVID-19 pandemic.
We are thrilled to announce that many of the ideas submitted are already underway at our hospital. Below are just a few of the exciting initiatives right here in Ottawa that will be receiving funding thanks to donor support of the COVID-19 Emergency Response Fund.
Using lab-grown human tissues to identify possible treatments
Dr. William Stanford
Dr. William Stanford and his colleagues are using human tissue models to understand why COVID-19 makes some patients severely ill. They also hope to identify and test new drugs that can reduce the severe lung damage that typically kills people with COVID-19. They will rapidly test two cellular pathways involved in causing this lung damage. They will then rapidly screen for drugs that have already been approved by Health Canada and the FDA that are able to block these pathways, and potentially reduce disease severity and death. Their research may also reveal biomarkers that can identify which patients with COVID-19 are most likely to require intensive care.
UPDATE: Funding provided by the COVID-19 Emergency Response Fund was used to put another technician on this project. The research team is looking at acute kidney injury and renal failure in COVID-19 patients. It is highly debated among nephrologists whether the renal involvement is due to primary or secondary effects. Researchers on this project used stem cells to grow kidney-like tissues called organoids in the lab. Using this model, they found that certain parts of the kidney are readily infected by a hybrid virus that mimics COVID-19. These data suggest that the kidney disease experienced by COVID-19 patients is likely due to infection of the kidneys. The team is working with collaborators in Toronto to infect these human kidney organoids with live virus and analyze the impact of the infection.
Stopping COVID-19 with behavioral science and artificial intelligence
Dr. Justin Presseau
Dr. Justin Presseau and colleagues plan to use state-of-the-art behavioural science and artificial intelligence to develop an app that can help people reduce how much they touch their eyes, nose and mouth. This T-shaped area of the face known as the T-zone is the main way that the COVID-19 virus gets into the body. Reducing T-zone touching could reduce the transmission of COVID-19, as well as transmission of other infections that pass through the nose and mouth. Most people touch their T-zone 15-20 times per hour, often without realizing it.
The app would help people become aware of this behavior and walk them through possible techniques and training to reduce T-zone touching. This project will involve international experts in machine learning and computer vision, health psychology and behaviour change, and human-centred design and infection control.
UPDATE: The research team led by The Ottawa Hospital and consisting of international experts in health psychology and implementation science are working on ways to support Canadians to reduce facial T-zone touching. They have identified several considerations that might influence this critical behaviour and the spread of disease. To coincide with flu season, they will be launching a national survey and conducting interviews with Canadians from coast to coast to improve their understanding of T-zone touching to inform the development of an additional protective strategy alongside physical distancing, handwashing, and wearing masks.
Understanding the challenge of COVID-19 for Ottawa’s most vulnerable people
Dr. Smita Pakhale
Dr. Smita Pakhale and her colleagues will harness the trust and engagement they have built with Ottawa’s most marginalized communities over the last 10 years through community-based participatory action research to examine how COVID-19 has impacted these individuals. Marginalized people who are low-income, homeless, and at-risk of homelessness face numerous social and health inequities that are exacerbated by crises like the COVID-19 pandemic. These individuals face unique barriers when accessing health services and may be last in line for support. Data co-collected and co-analyzed with people of lived experience could lead to the development of better policies and programs to help vulnerable populations during COVID-19 and future crises.
UPDATE: Since the funding announcement, researchers have completed the ethics approval process, and are now implementing the project at the Bridge Engagement Center (the Bridge), located in Vanier, Ottawa. The team is using a community-based participatory action research approach and have completed selection and training of community peer researchers with lived experience. These peer researchers have helped co-design surveys and interview guides. They are now actively recruiting project participants and collecting data at the Bridge via telephone, ensuring their safety. Preliminary findings are noteworthy, demonstrating more challenges faced by these most-marginalized communities as compared to pre-COVID-19. Researchers aim to complete the recruitment and data collection over the next few months which will also include semi-structured interviews about in-depth experiences during COVID-19, as well as a card-sorting exercise focused on COVID-19 media messaging. This approach ensures that those with limited literacy are still able to share their thoughts and experiences with the COVID-19 pandemic.
Mobile reporting of adverse events from a pandemic COVID-19 vaccine
Dr. Kumanan Wilson
Dr. Kumanan Wilson and his colleagues will harness their electronic vaccine-tracking platform CANImmunize to let Canadians report potential adverse events from a COVID-19 vaccine through their mobile device. This will be crucial in ensuring both the safety of a COVID-19 vaccine and enhancing public trust in the vaccine.
The team has already built and tested a proof-of-concept pilot app in partnership with the Canadian Vaccine Safety Network for monitoring adverse events from the seasonal influenza vaccine. This reporting function will be activated for testing during the fall flu season for use by participating employees at The Ottawa Hospital, in preparation for a probable COVID-19 vaccine in 2021.
Testing plasma from recovered COVID-19 patients as a possible treatment
Dr. Dean Fergusson
Drs. Alan Tinmouth and Dean Fergusson are contributing to the global effort to determine if plasma from people who have recovered from COVID-19 (called convalescent plasma) could be an effective treatment for actively infected patients. When someone becomes infected with COVID-19, their immune system develops antibodies against the virus. After they have recovered, these antibodies remain present in their plasma to shield them from possible future infection.
In theory, these antibodies could be transfused into people with an active COVID-19 infection, to help them fight off the virus. The trial will be conducted by the Canadian Transfusion Research Network in collaboration with Canadian Blood Services and Hema-Québec who will collect and test convalescent plasma in adults (CONCOR-1 study) and children (CONCOR-Kids study).
UPDATE: Proposed treatment: COVID-19 convalescent plasma (CCP) is the plasma collected from individuals who have previously contracted SARS-CoV-2 virus and COVID-19 disease and have developed neutralizing antibodies. The research team has partnered with Canadian Blood Services and Hema Quebec to solicit, collect, prepare and distribute CCP. This is a randomized clinical trial with 59 sites in Canada, three in New York City, one in Israel, and three in Brazil. The first patient was enrolled in May and there are now 425 patients enrolled with over 30 at our hospital. There have been no serious adverse events related to CCP reported to date and 2400 units have been collected and distributed across Canada. The trial will end in June 2021 and dissemination of results will happen in July 2021.
Predicting COVID-19 in populations
Dr. Doug Manuel
Dr. Doug Manuel and his colleagues in partnership with Ottawa Public Health have created an interactive website (613covid.ca) that predicts various scenarios around the number of hospitalizations and deaths in Ottawa due to COVID-19. The methods they are developing will help advance COVID-19 projections worldwide in addition to helping with local planning. They plan to refine their methods and develop better approaches to predict the effects of different levels of physical distancing. These projections will be invaluable in discussions around easing physical distancing restrictions.
UPDATE: Funds for this project were used to run the 613covid.ca website. This research team is unique in Canada — and one of the few worldwide — to provide daily, automatically generated covid-19 projections. There have been over 100K views of the projections since it launched in the spring. The program has expanded to include:
long-term and short-term projections for cases and hospitalizations.
first-in-Canada wastewater surveillance and modelling.
SCRiPS – an online calculator that public health experts can use to help develop COVID-19 screening and testing protocols.
Repurposing existing drugs and finding new ones
Dr. Jean-Simon Diallo
Dr. Jean-Simon Diallo and his colleagues have developed a novel “bio-sensor” that can identify drugs that block the COVID-19 virus from attaching to cells, thereby preventing infection. First, they plan to test this novel approach on a library of more than 1,000 small molecules that have been approved to treat other diseases. Then they will attempt to identify novel antivirals drugs from a library of more than 200,000 small molecules.
UPDATE: This project aims to identify antiviral drugs that can help in the fight against coronavirus. The research team has developed a novel biosensor allowing them to test the effects of hundreds of thousands of drugs in this capacity. The first step aimed to identify potential antivirals from a collection of over 1000 currently approved drugs that may be repurposed as antivirals. They have identified one leading candidate drug from this collection which is a common antifungal and that appears to block the interaction between SARS-CoV-2 and the protein to which it normally binds to enter and infect cells. The next steps are to directly test this drug on coronavirus through collaboration with other researchers in Canada and expand testing to a much larger collection of new potential drugs.
The projects currently underway are just the beginning. In the coming weeks, additional COVID-19 Emergency Response Fund grants will be awarded for research, as well as for the development of innovative treatments and creative new ways to combat the virus. But our work is not yet complete. We need donor support to ensure the COVID-19 Emergency Response Fund can continue to support front-line medical teams, provide essential equipment, and contribute to the care and comfort of patients.
Keep checking back for more updates on how donations are being put to work right away and are making a difference in The Ottawa Hospital’s fight against COVID-19. To get regular updates sent directly to your inbox, sign up for our newsletter, Vital Links.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: COVID-19, World-Leading Research
APRIL 29, 2020 OTTAWA, ON – The Ottawa Hospital’s COVID-19 Emergency Response Fund received a significant boost thanks to the generosity of a $100,000 match gift from the Nanji Family Foundation.
“The Ottawa Hospital Foundation is incredibly grateful to have the support of the Nanji Family Foundation and we look forward to seeing how their gift will inspire others to give,” said Tim Kluke, President and CEO, The Ottawa Hospital Foundation.
The COVID-19 Emergency Response Fund will help patients and staff directly affected by the COVID-19 pandemic. Donations made will be matched by the Nanji Family Foundation and will:
support our frontline medical teams
purchase specialized protective equipment
develop innovative treatments through highly specialized technology
contribute to the care and comfort of patients
support our scientists and our researchers in their efforts to combat COVID-19
As the pandemic continues to evolve, incredible stories of generosity continue to emerge. Our front-line healthcare team has to adapt quickly and this match gift of up to $100,000 will help to keep them safe, along with our patients. It will also help support the work of our researchers who have joined the global fight against COVID-19. The Nanji Family Foundation has donated a total of $1.6 million to 16 hospitals across Canada in this collaborative effort.
We’re grateful to have the support from our community and thank the Nanji family for their leadership and for inspiring others to give and double their impact.
About The Ottawa Hospital:
The Ottawa Hospital is one of Canada’s top learning and research hospitals, where excellent care is inspired by research and driven by compassion. As the third-largest employer in Ottawa, our support staff, researchers, nurses, physicians, and volunteers never stop seeking solutions to the most complex healthcare challenges.
Our multi-campus hospital, affiliated with the University of Ottawa, attracts some of the most influential scientific minds from around the world. Our focus on learning and research leads to new techniques and discoveries that are adopted globally to improve patient care.
We are the Regional Trauma Centre for eastern Ontario and have been accredited with Exemplary Standing for healthcare delivery — the highest rating from Accreditation Canada. We are also home to world-leading research programs focused on cancer therapeutics, neuroscience, regenerative medicine, chronic disease, and practice-changing research.
Backed by generous support from the community, we are committed to providing the world-class, compassionate care we would want for our loved ones.
For more information about The Ottawa Hospital, visit ohfoundation.ca.
As the COVID-19 pandemic continues to evolve, experts at The Ottawa Hospital and healthcare partners throughout the region have geared up to stop the spread of this infectious disease. From our crisis preparedness plan, to COVID-19 research already underway, we have the knowledge and experience to tackle this pandemic head-on. Our researchers are harnessing their unique expertise and exploring more than 50 COVID-19 research projects to help in the global fight against this virus.
All of the COVID-19 simulation exercises and research projects being explored at The Ottawa Hospital will make use of shared research equipment, resources, and facilities that have been developed over many years, thanks to generous support from our community.
“Thanks to generous support from the community over the years, we’ve been able to develop unique research facilities and technologies that we are now rapidly applying to the fight against COVID-19,” said Dr. Duncan Stewart, Executive VP Research, The Ottawa Hospital. “Similarly, today’s community support for research means we will be ready for tomorrow’s health challenges, whatever they may be.”
Calming the immune system in critically ill patients
Dr. Stewart is leading a team of researchers working to launch a clinical trial of mesenchymal stromal cells (MSC) therapy for COVID-19 patients with Acute Respiratory Distress Syndrome (ARDS).
The immune system plays a crucial role in defending the body against COVID-19, but sometimes it can become overactivated, resulting in severe damage to the lungs, called ARDS. In COVID-19 patients, ARDS is the major cause of severe illness and death.
Studies have shown that mesenchymal stromal cells (MSCs) can dampen an overactive immune response and help patients with ARDS related to other kinds of infections. Our researchers will build on their extensive experience in manufacturing MSCs and leading the world’s first clinical trial of MSCs for septic shock. This project will likely involve partners in Ontario and Europe, working in a concerted effort to find novel therapies to improve outcomes in COVID-19 patients.
Repurposing existing drugs and finding new ones
Dr. John Bell in his lab at The Ottawa Hospital. His team could use their virus manufacturing expertise in the production of a vaccine for COVID-19.
Other researchers of The Ottawa Hospital and the University of Ottawa are looking to identify already-existing drugs and their potential effectiveness in treating patients with COVID-19. Drs. Taha Azad, Ragunath Singaravelu, Jean-Simon Diallo and John Bell have developed a novel system known as a bio-sensor that can identify small molecule drugs that block the COVID-19 virus from attaching to cells, thereby preventing infection. First, they plan to test this approach on a library of more than 1,000 small molecules that have been approved to treat other diseases. They will then attempt to identify antiviral drugs that could be effective in treating this virus.
Learning from our COVID-19 patients and testing therapies
Researchers from around the world are sharing their experiences and findings and are working together to determine the best approach to treating patients with COVID-19.
To help with this global effort, infectious disease researchers at The Ottawa Hospital and the University of Ottawa are working locally to create a registry of COVID-19 patients in our community. Under the leadership of Dr. Michaeline McGuinty and Dr. William Cameron, the researchers plan to look for patterns among cases and determine how well treatments are working. They will also use blood samples to study the virus and the body’s response to each treatment.
“Thanks to generous support from the community over the years, we’ve been able to develop unique research facilities and technologies that we are now rapidly applying to the fight against COVID-19.” – Dr. Duncan Stewart, senior scientist in the Regenerative Medicine Program and professor at the University of Ottawa
Working towards a vaccine
While some researchers work to find better treatment options for COVID-19, Dr. Carolina Ilkow, Dr. John Bell and their team of experts in making cancer-fighting viruses at The Ottawa Hospital are working hard to develop a possible vaccine, in partnership with scientists and clinicians in Canada and around the world. The vaccine would contain small parts of genetic material from the COVID-19 virus, embedded into a different virus that does not cause human disease. This replicating viral vaccine would also produce its own adjuvant – a substance that stimulates a stronger immune response, resulting in a more effective vaccine. Once a promising vaccine is created, the team will be able to make large quantities in The Ottawa Hospital’s Biotherapeutics Manufacturing Centre. This facility is the only hospital-based lab in Canada capable of producing virus-based vaccines and therapies for clinical trials.
Nurses at the COVID-19 Assessment Centre prepare a swab to be transported to the lab and tested for COVID-19.
Putting preparedness to the test
While our researchers have been nimble in responding to COVID-19 The Ottawa Hospital was already planning for the possibility of a future pandemic long before this virus appeared. When it comes to preparing for the worst, we are leading the way in developing strategies to effectively manage a crisis.
The intensive care units (ICU) at both the General and Civic campuses, where the most acutely ill COVID-19 patients will be treated, will triple their current size should we need the room. If these become over capacitated, the hospital would make use of other existing hospital facilities to increase its ability to care for severely ill patients.
Eastern Ontario hospitals are also working together to create a regional patient flow strategy to care for patients. Hospitals will transfer COVID-19 positive patients who need acute or critical care to select hospitals for treatment. Patients who do not require this level of care will be transferred out of acute or critical care hospitals to the most appropriate hospital setting. This will ensure that our healthcare system does not become overwhelmed by the COVID-19 outbreak.
Simulation exercises save lives
Transferring patients from the Emergency Department to the ICU is no easy feat in a 100-year-old hospital. It’s for this reason, the University of Ottawa Skills and Simulation Centre have readied staff by running simulation drills and tests.
The drills, which made use of a high-tech mannequin capable of sneezing, are designed to refine the safe treatment and transport of a severely-ill patient experiencing respiratory failure.
Simulations are vital as they allow staff to practice their skills in a real-time environment make adjustments if necessary, and ultimately provide better care to patients. Similar to the Code Orange simulations, which took place two months before the Westboro bus crash on January 11, 2019, this type of hands-on training further prepares staff on the frontlines.
On November 16, 2018, The Ottawa Hospital underwent a Code Orange emergency response exercise as part of ongoing preparedness to respond effectively to a disaster in the community. Participating in such a training exercise meant staff would be even more prepared should a real Code Orange be called.
Just two months later, a double-decker bus crashed into the Westboro bus station. Thirteen severely-injured patients were subsequently transported to the Emergency Department. The simulation exercise helped to ensure that The Ottawa Hospital staff were even more prepared to save their lives.
Community support essential
A strong hospital requires the support of its community and that couldn’t be more true than during these unprecedented times. You can support world-class care and ground-breaking research that is saving lives every day.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Biotherapeutics, COVID-19, TOH Family, World-Leading Research
Published: March 2026
Dr. Innie Chen
Dr. Innie Chen
Dr. Innie Chen is the new Dr. Elaine Jolly Chair in Women’s Health and Gynecology Research — a chair supported by donors and established to honour Dr. Jolly’s pioneering work to advance women’s health.
A national leader in gynecologic surgical research, Dr. Chen also treats women who have complex gynecologic conditions. She is currently leading national collaborations, and her research is focused on issues surrounding equity of surgical care, safety, and raising the quality of care for women’s gynecologic health.
Her work has already informed national clinical guidelines, reduced surgical complications, and improved recovery for thousands of patients.
Dr. Chen’s focus for the future is harnessing the power of artificial intelligence and big data to predict surgical risks and address health inequities, opening new methods for more personalized care and overcoming invisible barriers in health systems.
Dr. Natasha Kekre
Dr. Natasha Kekre
Dr. Natasha Kekre has just been announced as the new Program Director of our Cancer Research Program!
In 2023, she was awarded the Research Chair in Advanced Stem Cell Therapy and has been gaining national attention for her work in bringing lifesaving therapies to Canadian cancer patients. In fact, her work in immunotherapy helped earn her the 2023 Joe Doupe Young Investigator Award.
Her early-career work secured millions in funding and led to numerous peer-reviewed publications, but she might be best known for her pioneering work building the first “made-in-Canada” (CAR) T-cell clinical trial.
“Creating a made-in-Canada cell therapy platform has been groundbreaking and opens a world of possibilities for Canadians needing life-saving therapy options,” says Dr. Kekre.
Rita Timpano
Rita Timpano has been a nurse at TOH for more than 34 years and is currently an RN in the surgical suites, where she greets patients before they come into the operating room. She prepares them for their surgery and usually stays with them as they go off to sleep.
“I hold their hand, and I reassure them, as they’re often anxious,” says Rita. “Then, I proceed with the surgery aspect. If I’m in a scrub role, I assist; if I’m in a circulating role, I do everything in the room to prepare. Patient safety is the number one priority.”
Rita is known for being supportive and compassionate — words she also uses to describe her fellow colleagues. But Rita’s kindness has not gone unnoticed, and recently she received a special thank you, in the form of a Gratitude Award, from a patient, who had this to say to Rita:
“A ‘thank you’ is not enough. Last fall, you treated my father like he was your family. Your sense of humour and the fact that you could speak to him in Italian immediately put him at ease, and I knew I was leaving him in good hands at the OR doors. This past June, it was my turn. Your hug before I entered the OR and you holding my hand as I drifted off to sleep are things I will never forget. Thank you for your kindness, your empathy, and your smile.”
Rita Timpano
Dr. Lisa Caulley
Dr. Lisa Caulley
Dr. Lisa Caulley is a clinician-scientist and otolaryngologist-head and neck surgeon at The Ottawa Hospital.
Her journey into science was inspired by the desire to understand the unknown and the possibilities that science can bring to the world in general. She sees it as a space that combines creativity with curiosity, where asking questions, thinking differently, and testing ideas can lead to discoveries that have real-world impact. That freedom to explore and create is what keeps Dr. Caulley inspired.
Along the way, supportive mentors and meaningful research experiences showed her how powerful science can be when it’s driven by purpose. And that sense of impact and the freedom to explore and create is what keeps her motivated to this day.
Dr. Caulley also hopes to inspire other young women to pursue a career in science. Her advice is: “Stay positive and don’t be afraid to fight for your voice to be heard. Find mentors who support you and remember that there’s no single “right” path into science.”
Dr. Kathleen Gartke
Pioneering orthopedic surgeon and leader in Canadian medicine, Dr. Kathleen Gartke, has recently been appointed to the Order of Ontario — the province’s highest honour. This prestigious recognition speaks volumes about her lifelong commitment to patients, innovation, and leadership — and it also reflects the remarkable standard of excellence we are fortunate to have at The Ottawa Hospital.
Dr. Gartke began her outstanding career as an orthopedic surgeon at Ottawa’s Grace Hospital in 1984 and joined The Ottawa Hospital in 1999. For 15 years, she was the only operating female orthopedic surgeon in Ottawa. She retired from her surgical practice in 2016 before joining the hospital’s administration as Senior Medical Officer, a position she held until October 2025. From then until retirement at the end of February 2026, she served as Strategic Medical Advisor.
In addition to producing a large body of research during her career, for more than 45 years, Dr. Gartke has been a member of the Federation of Medical Women of Canada (FMWC), where she served on the National Executive team for 12 years.
Since joining the administration at The Ottawa Hospital, Dr. Gartke has driven quality and safety initiatives, earned an Award of Excellence and championed women’s health through national campaigns and mentorship.
Dr. Kathleen Gartke
We’re grateful for Dr. Gartke’s tremendous work as a surgeon, and for advancing patient care and women’s leadership in medicine in Ottawa and across Canada.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Patient Care, TOH Family, World-Leading Research
For an update on Marcie’s story, click here to see how far Marcie has come.
It was a bitter cold, winter day on Friday, January 11, 2019. Marcie Stevens was making her way home to Kanata for the weekend from downtown. The Public Safety employee sat on the second level of a double-decker OC Transpo bus when it crashed into the overhang of the Westboro transit station. It was 3:50 p.m.
Ten minutes away from where the crash occurred, the trauma team at The Ottawa Hospital was alerted, and a Code Orange was called. The Emergency Department began clearing space, and a large number of staff converged including surgeons, nurses, anesthetists, emergency physicians, and support staff. A massive team of about 150 people would await the injured passengers. At 4:28 p.m., the first patient arrived at The Ottawa Hospital’s Civic Campus, home to the only level 1 trauma centre for adults in eastern Ontario. In total, 13 severely injured patients over a two-hour period were rushed to the trauma centre – one of the injured was Marcie Stevens.
Calm amidst chaos
The married mother of two recalls being conscious and considerably calm throughout the entire ordeal. Though she was pinned on the top level of the bus and critically injured, she was able to call her husband, Christopher, to tell him she couldn’t pick up their children. She even thought to call work to let them know she wouldn’t be in on Monday and was able to help to calm those around her while emergency crews worked furiously to remove them from the wreckage. Marcie would need that calm composure in the midst of adversity for what awaited her.
“I couldn’t have gotten this far without the incredible people and support from The Ottawa Hospital – from the trauma team to the ICU to the Rehab Centre – it’s incredible. Compassionate is the best word to describe it.” – Marcie Stevens
The trauma team was ready
After arriving at our Emergency Department, Marcie recalls she had lost so much blood and that after her CT scan her blood pressure began to plummet, but the trauma team was ready. “The nurse in the Emergency Department had the O negative blood in her pocket. They immediately started pumping blood back into my system. My blood pressure stabilized, and I was then rolled into the operating room. The only time I passed out was when they put the mask on to put me to sleep.”
(From left to right) Dr. Ian Grant, Dr. Peter Glen, Dr. Maher Matar and Dr. Jacinthe Lampron.
Marcie would wake up on Sunday morning, groggy and swollen. That’s when she learned from her husband that both of her legs had been amputated. “I knew going into the operation that my left leg was gone, because they told me. But they were going to try to save the right leg, but they couldn’t, and on Saturday they had to take it.”
While a completely new world awaited Marcie, her positive attitude never wavered. “You adapt and that’s what I have been doing. This is the way it goes. I couldn’t have gotten this far without the incredible people and support from The Ottawa Hospital – from the trauma team to the ICU to the rehab centre – it’s incredible. Compassionate is the best word to describe it.”
Waking up to a different life
Soon after the bus crash, Dr. Nancy Dudek, Medical Director, Amputee Program at The Ottawa Hospital Rehabilitation Centre, met Marcie at her bedside for the first time. “I had regular visits with Marcie when she was in the trauma unit to determine when she would be medically ready to come to the Rehab Centre.” Our Rehabilitation Centre specializes in the physical rehabilitation of those who have experienced a disabling physical illness or injury. It serves the residents of eastern Ontario.
Dr. Dudek is quick to point out though that Marcie’s rehab started soon after she was admitted to the hospital. “We started rehabilitation plans when she was still in the Trauma Unit. She was a very avid participant of early rehab.”
Marcie Stevens and her family.
Marcie’s road to a new way of living life began with her multi-disciplinary care team helping to get her wounds healed. That would lead to teaching her how to move independently once again.
By the end of February, Marcie moved to The Ottawa Hospital’s Rehabilitation Centre. She says the staff were incredible from the moment she arrived. “I was in a room with three other women. They put the two who fell asleep early on one side and me and an older patient – the night owls – on the other.”
It was during rehabilitation that Marcie learned how to transfer from the bed to her wheelchair without a lift. She learned how to cook in a kitchen that is not accessible, to prepare for her return home, and she’s learning how to drive with hand controls.
Preparing to go home
Dr. Dudek explains there’s a great deal to cover in rehab. “We teach wheelchair skills, including what the right wheelchair is for the patient. We also had to work on strengthening, including core strengthening. Then, we talked about what would be the immediate needs to get her home to her family, including her five and 12-year-old boys.”
Westboro bus crash double amputee, Marcie Stevens, doing strength testing in the rehabilitation centre at The Ottawa Hospital with Dr. Nancy Dudek.
Marcie went home on Friday, April 12, 2019. Three months after arriving at the hospital. When Marcie reflects on her feelings as she was leaving the rehab centre, she takes a moment and then replies, “It was a giddy day. It’s not like I didn’t like the Rehab Centre,” she quickly qualifies her response smiling at Dr. Dudek, “but it was good to be home with the kids.”
Of course, going home didn’t mean Marcie’s rehabilitation was over, but it was a major advancement in her recovery – a recovery that she faced head on with a resilience that never wavered. Dr. Dudek says it’s been inspiring to watch Marcie over the last year. “She is an incredibly positive person. That has been consistent. It’s something that was there right from our first meeting and it hasn’t really faded. She has a ton of energy and other people really gravitate towards her. She’s very popular around here.”
“Rehab is great. It is the jewel of the hospital that nobody knows about. They are sort of hidden away here. They have to deal with so many types of injuries and states of mind. Not everyone at the centre is accepting of what happened to them,” admits Marcie.
As Marcie recounts all that she’s been through in the past year, she still jokes and laughs. When Dr. Dudek is asked if she thinks this incredible attitude helped with Marcie’s recovery, the answer comes fast. “One hundred percent. She has made significant changes and implemented new things to her life. It’s very impressive to see. We can show people the way, but we can’t do it for them.”
Moving forward
Today, Marcie and her family are moving forward. A new home is necessary – one that is fully accessible, and Marcie talks about getting back to work someday.
She misses her colleagues, but she knows that day will come with time. “I’m a very positive person and it will take time to get used to the changes in my life, to adjust to having no legs. It’s difficult. I’ll get there.”
For now, she will continue with her regular rehab. Eventually she will only need annual visits. For now, her weeks are filled with trips to the gym and the pool, all to get her stronger for the new world she faces. Despite the challenges, she embraces it all with confidence, a smile, and you could say a bit of attitude as she wheels away wearing her black leather jacket, sunglasses, and a streak of pink in her hair.
Update: Two years later
Marcie Stevens with her prostheses.
Today, Marcie is learning to walk again thanks to her new prosthetics. While the pandemic has caused some delays in her progress, she’s hopeful the spring will bring more good news. “I am looking at procedures to help me move easier in my prosthesis after significant weight loss,” says Marcie. She’s lost 60 pounds in an effort to better adapt to using her prosthetic legs.
In the springtime, Marcie is optimistic that she will have a chance to trial powered knees, which will allow her to move better when she sits down and stands up. She’ll also have her adapted vehicle, to help her shuttle her boys around town. In two years, Marcie has come a long way. While her recovery continues, our rehab team is with her as she takes each new step forward.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Creating Tomorrow, Rehab, Trauma
A race against the clock
Karen Lawrence is no stranger to helping those in need. After all, she’s a Clinical Manager of Oncology at The Ottawa Hospital. Her position, largely characterized as providing specialized treatment and care to some of the hospital’s most ailing, has taught her the value of advocating for those in need and raising money for critical research.
Now, sitting with the knowledge that her own body will soon start to deteriorate, she reflects on her life – and the future of her three boys.
An uncertain future
On January 27, 2014, Karen received the results of a genetic test, confirming one of her biggest fears. She is a carrier of a gene that causes amyotrophic lateral sclerosis (ALS) – a rare disease that gradually paralyses people because their motor neurons, which send signals from the brain to the muscles, break down and die.
As she sits staring at an oversized clock mounted on her living room wall, it seems to take on more significance – each second that passes moves Karen toward her inevitable fate. Like so many family members before her, Karen will too develop the disease. It’s just a matter of time.
“My family has been stricken with the familial form of ALS,” she explains with a pained expression. “I have lost 14 members of my family to this devastating disease, including my father.”
Watching ALS render her father helpless, while keeping his mind intact, was a cruel reminder that today there is no fighting this disease. “There is little hope yet. Today, there is only pain and suffering. Facing an uncertain future, a cure can’t come soon enough,” says Karen.
Results of a genetic test showed Karen Lawrence carries a gene that causes ALS.
Family ties
No one in Karen’s family realized it at the time. Several members of her extended family were diagnosed with ALS and passed before they connected the dots. It was only once her grandfather, uncle and father were diagnosed that the family started to talk about the fact that it was likely genetic. The women in her family, her aunt and cousins, were diagnosed in their 40’s. The men were diagnosed when they were a little older, but under the age of 60. Once diagnosed, most only survived 12-18 months.
With a 50/50 chance of having the gene, it was never far from Karen’s mind. “It’s like walking around with a target on your back. You’re just kind of waiting,” she said. And she was tired of it – the waiting. That’s when she got tested.
“It’s like walking around with a target on your back.” – Karen Lawrence
“When they told me I had the gene, I was very composed and held it together until I thought of my kids and then I started to cry. That’s when it really hit me. I potentially gave a terminal illness to my children. So that’s very difficult to live with.”
The race is on
When Karen found out that she had the gene, something as simple as dropping a pen, or a small stumble, would have her mind racing to the future.
Karen is aware that it’s just a matter of time before her brain will no longer be able to talk to her muscles. Eventually, she’ll have trouble with her balance, then she won’t be able to walk, then talk and then eat. But her mind will be intact, trapped within her body, while she waits for ALS to take her ability to breathe. Karen has a pretty clear idea of what this will look and feel like, having watched her father go through it just a few years ago.
So, how does she grapple with the thought of such a grim future? She runs – literally. And she raises a substantial amount of money in support of neuromuscular research and care while she’s at it.
Her first ever marathon was in Copenhagen and her second in New York City. More recently, she has participated in The Ottawa Hospital’s Run for a Reason, where alongside her team, she raised funds towards a brand-new Neuromuscular Centre right here in Ottawa.
“The race is on to fund research to find a cure, or to prevent onset before my three beautiful boys are faced with the same agonizing decision of whether to get tested.” – Karen Lawrence
Drs. Jodi Warman Chardon and Robin Parks were instrumental in establishing the NeuroMuscular Centre, which opened in 2018.
Karen Lawrence is the Clinical Manager of Oncology at The Ottawa Hospital.
A new Neuromuscular Centre
Thousands of people in eastern Ontario are affected by neuromuscular diseases. Until recently, patients had to travel to Montreal or Toronto to participate in clinical trials to help further research in these diseases. However, Dr. Jodi Warman Chardon noted that The Ottawa Hospital had more than 50 researchers and clinicians working on behalf of people like Karen. Each is working on various aspects of neuromuscular disease – from clinical care to lab research. There was no reason why the most promising clinical trials couldn’t be offered here in Ottawa.
Dr. Warman teamed up with Senior Scientist Dr. Robin Parks, who is conducting lab-based research on neuromuscular diseases. Their dream to have a centre that would bring these experts together in one place caught traction, and in May 2018, The Ottawa Hospital Neuromuscular Centre opened its doors to patients. “What’s exciting is it’s more than just a clinic. It’s a clinical research centre,” said Dr. Robin Parks. “So the idea is to do research and get results that will then feed back to the patient to provide insight into new therapies for them.”
Today, Ottawa is at the global epicenter of neuromuscular research. Equipped with the strongest neuroscience research team in the world, we are well positioned to discover new treatment options and cures, which will change patient outcomes worldwide.
“When a cure is found for this disease [ALS], the chances are it will be found in Ottawa,” said Duncan Stewart, Executive Vice President, Research, The Ottawa Hospital.
Zest for life
Karen does not yet have ALS, so she is not undergoing any treatment. But she remains hopeful that when she develops the disease, she will participate in the Neuromuscular Centre’s clinical trials and benefit from treatment developed at The Ottawa Hospital.
Until then, she tries to not dwell on what lies ahead and instead focuses on her hope for a healthy future for her boys.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.
Categories: Clinical Trials, World-Leading Research
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.