Minimally invasive surgery ‘perfectly’ restores hearing
After a brain tumour began growing in to his ear, Denis Paquette was at risk of losing his hearing in both ears – a circumstance that would strip him of his ability to hear his wife’s voice forever. With traditional brain surgery deemed too risky, Dr. Fahad Alkherayf and Dr. Shaun Kilty were challenged to find a safer solution – removing the tumour through his nose.
A life unlike most
Since birth, Denis Paquette, now 66, has been deaf in one ear. It’s clear he has a deep-rooted understanding of the nuances of having such an impairment. After all, it’s all he’s ever known. Holding the phone to his good ear and turning his head while in conversation to better hear someone are habits he was quick to establish.
But in 2016, these little tricks, which he has cultivated throughout his life, started to fail him. Conversations were getting harder to hear and Denis’ wife, Nicole,

noticed that Denis was progressively increasing the volume on the television.
“I was beginning to be frustrated because people were talking to me, but I was just getting parts of the conversation,” said Denis.
Journey to diagnosis
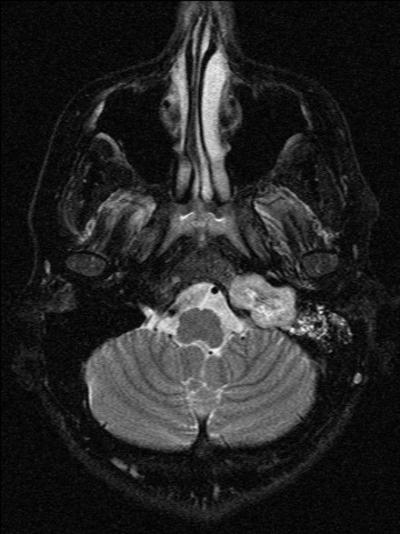
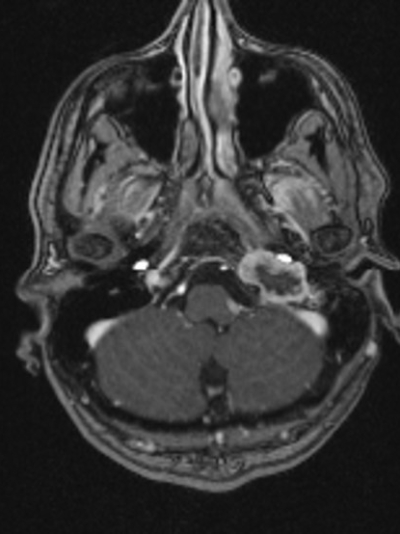
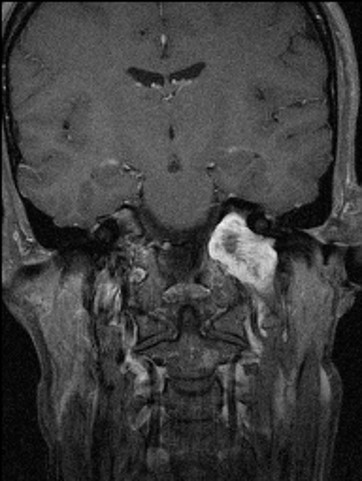
Concerned about his hearing, Denis visited his family doctor. He was sent for various hearing tests, each showing that something was wrong. It was then that Denis was referred to Dr. David Schramm, a hearing specialist at The Ottawa Hospital. Dr. Schramm ordered an MRI that revealed Denis had a rare tumour growing in his skull and in to his inner ear. These weren’t the results Denis and Nicole were expecting.
“I didn’t know what to expect, so it was really shocking news,” said Denis.
Denis needed specialized surgery to remove the tumour and required the expertise of neurosurgeon Dr. Fahad Alkherayf and ear, nose, and throat (ENT) specialist Dr. Shaun Kilty.
Due to the complexity of Denis’ diagnosis, Dr. Alkherayf and his team were challenged to remove the tumour without jeopardizing his hearing completely.
“The tumour was growing in his skull and in to his inner ear, putting pressure on his hearing nerve on the good ear. There was a risk he would lose the rest of his hearing,” said Dr. Alkherayf.
“Despite it being a benign lesion, the impact of it was huge.” – Dr. Fahad Alkherayf
Dr. Alkherayf knew that removing the tumour through Denis’ ear could risk permanently damaging what little hearing he had left. With this in mind, Dr. Alkherayf recommended that Denis undergo the newly-available minimally invasive brain surgery. With this technique, his tumour would be removed through his nostrils instead of through his ear.
The risk was high
Traditionally, brain surgery for a case such as Denis’ would take place through the ear and require a large incision through the skull. But with only one good ear to start with, performing brain surgery in this way could permanently and completely impair his hearing.
Not only could Denis lose his hearing, the traditional method of removing such a tumour has a greater risk of complication, a higher chance of infection, and demands a longer recovery period – up to six months. It would also leave a large scar, beginning in front of his ear and extending all the way up and behind it. The thought of undergoing such a procedure alone was nerve-racking.
A new surgery technique
Over the last several years, Dr. Alkherayf has advanced new techniques for removing various types of brain tumours, known as minimally invasive surgery.
Minimally invasive surgery has transformed the way operations are performed by allowing surgeries to be carried out as keyhole procedures, a surgical procedure that provides access to parts of the body without having to make large incisions. This operation is much safer, with risk of infection and recovery time greatly reduced. In many cases, patients are discharged within just a few days of surgery.
“It’s quicker to recover for patients,” said Dr. Kilty. “Because they don’t have to recover from the extensive dissection that traditional approaches [surgeries] require.”
Performing these types of surgeries requires two physicians – a neurosurgeon to remove the tumour and an ENT to provide access to the tumour through the nose and to control the endoscope. Due to the complex nature of these surgeries, Dr. Alkherayf is among a small group willing to perform them. Many are looking to The Ottawa Hospital to learn about this innovative surgery. “We have become one of the top places in Canada for this technique,” said Dr. Alkherayf.

“They did a miracle on me”
On July 20, 2016, Denis underwent a five-hour operation during which Dr. Alkherayf and Dr. Kilty were able to successfully access and remove the tumour through his nose. The insertion of a microscopic tube that would travel from the cavity of where the tumour once was to his sinuses which would prevent future buildup of fluid and prevent the chance of reoccurrence.
When he woke up, Denis was astounded that he could hear his wife’s voice. “I woke up and wow,” said Denis, “I could hear!”
Just two days after his surgery, he was discharged.
“They did a miracle on me. They did something fantastic,” said Denis, whose hearing tests have been perfect ever since.
“They did a miracle on me. They did something fantastic.” – Denis Paquette
Thanks to the care Denis received at The Ottawa Hospital and the benefits of minimally invasive surgery, he can now enjoy watching his television shows and conversing with his wife without issue. He no longer fears a life without sound.
The Ottawa Hospital is a leading academic health, research, and learning hospital proudly affiliated with the University of Ottawa.