Category: Creating Tomorrow




September 22, 2023, OTTAWA, ON – Jennifer Van Noort, Vice-President of Philanthropy at The Ottawa Hospital Foundation was recognized for her leadership in our community at the annual gala hosted by Women’s Business Network. Van Noort won in the Accomplished Category for Enterprise Leaders. This recognizes women who work for for-profit, not-for-profit, non-governmental organizations, social enterprises, a charity, or a foundation.

In a true testament to Van Noort’s leadership, she was deeply moved by the recognition. “Receiving this award is both an honour and a reminder — that it takes passion, purpose, and a united community to drive real change. Every day, I have the privilege to work with donors who are passionate about supporting The Ottawa Hospital’s mission to provide world-class care, and I couldn’t do what I do without the entire team at the Foundation who works tirelessly to help make that mission a reality.”
Over the last two decades, Van Noort’s leadership has been an invaluable asset to The Ottawa Hospital Foundation where she is an integral part of the $500-million Campaign to Create Tomorrow. Tim Kluke, President and CEO of The Ottawa Hospital Foundation, celebrated this incredible honour. “Jennifer is standing alongside an elite group of changemakers — and our team couldn’t be prouder. Her impact not only on our Foundation, but also in the community is immeasurable, and her passion and positivity continue to inspire us all.”
For Van Noort, the success she’s experienced is thanks to the generosity of donors and the relationships she’s built over her lengthy career in philanthropy. “I believe at the heart of fundraising is relationship building. Making connections, earning trust, and having the most genuine dialogue possible. It is what informs every aspect of what I do. I also believe that’s why we’ve seen the success we have to date with our historic campaign.”
Van Noort takes the recognition to heart as she and the Foundation team move forward with the campaign that currently stands at $294 million raised.
To join the Campaign to Create Tomorrow in support of The Ottawa Hospital, visit CreatingTomorrow.ca.
About The Ottawa Hospital:
The Ottawa Hospital is one of Canada’s top learning and research hospitals where we are guided by our vision to provide the world-class and compassionate care, we would all want for our loved ones. Our multi-campus hospital, affiliated with the University of Ottawa, is home to the Regional Trauma Centre and Cancer Centre, and to discoveries that are adopted globally.
Backed by generous support from the community, we are focused on reshaping the future of healthcare to improve the health of our diverse population of patients from eastern Ontario, western Quebec, and Nunavut.
For more information about The Ottawa Hospital, visit OHFoundation.ca.
-30-
Published: September 2023
Before January 2008, Georges Gratton and Jeannine Constantin’s family hadn’t needed The Ottawa Hospital. Living in Boucherville, Quebec and then in the Outaouais region of western Quebec, they had always received care at their local hospitals and clinics. But when their grown daughter, Geneviève Gratton, was diagnosed with acute lymphoblastic leukemia, she needed specialized care and was transferred to The Ottawa Hospital within one day of her diagnosis.

Specialized care for patients from western Quebec and beyond
This scenario is not unique to Geneviève’s case. In fact, The Ottawa Hospital regularly provides care that extends well beyond the city’s borders, and one quarter of our patients live in a rural area.
Many patients from the Outaouais region choose to or need to come to The Ottawa Hospital, particularly the Emergency Department for care, or like in Geneviève’s case, for specialized cancer care that they are unable to access closer to home. In addition to those who travel from western Quebec, patients also come from across eastern Ontario and as far away as Nunavut. At times, people from coast to coast come to our hospital for care they can’t get anywhere else.
“Our hospital is uniquely positioned to provide care for patients coming to us from far and wide and with a wide range of needs.”
— Suzanne Madore
According to Suzanne Madore, Chief Operating Officer and Chief Nursing Executive, The Ottawa Hospital plays an important role in healthcare delivery in Ottawa and beyond. “Our hospital is uniquely positioned to provide care for patients coming to us from far and wide and with a wide range of needs,” she says. “We have also worked hard to develop multiple collaborative partnerships within the region that provide our patients with access to specialized services.”
Diagnosis leads to stem cell transplant
While this was the first time Geneviève needed our hospital, she was grateful to be receiving the specialized cancer care she needed. At the time, she was working as a notary in Quebec and was a busy mom of three young children — aged 9, 6, and 1 — when her spleen suddenly ruptured.
A month later, she and her husband, Jean-François, noticed she wasn’t healing properly from the surgery to her spleen. She was incredibly weak and pale and was also experiencing a host of other symptoms including red spots all over her body (petechiae), constant nightmares, and fevers.

“My husband brought me to the Hull hospital on two occasions, and when they were taking my blood during one of those visits, my blood started gushing out like a fountain,” recalls Geneviève. “A hematologist took a biopsy and found out it was leukemia.”
Within 24 hours, Geneviève was transferred to The Ottawa Hospital where her specialized care began right away.
Family rallies following leukemia diagnosis

Geneviève’s entire network of family and friends immediately came together to support not only her, but also her husband and her children throughout this ordeal.
“It was like a net unfolding to protect and support me.”
— Geneviève Gratton
After her initial treatment, her medical team said that she needed an allogeneic stem cell transplant, meaning the stem cells needed to come from a donor, rather using Geneviève’s own stem cells. Fortunately, one of Geneviève’s two siblings, her sister Julie Gratton, was a perfect match, and she didn’t hesitate to donate her own stem cells to help save her little sister.
“Although I feared the whole thing, I would do the same if Geneviève would need it again. I was reassured by The Ottawa Hospital on the process of what I would have to do to give my stem cells. It wasn’t painful, and I was well treated” says Julie.
“I would do the same if Geneviève would need it again.”
— Julie Gratton
For Geneviève’s parents, it was a frightening time with a rollercoaster of emotions. They were worried for her and the seriousness of her diagnosis and also deeply grateful that Julie was a match and willing to donate her stem cells. As the transplant date approached, the entire family anxiously waited and hoped for the best.

Stem cell excellence at The Ottawa Hospital
Thankfully, Geneviève was in the most capable hands. In fact, The Ottawa Hospital is a major centre for the growing area of stem cell transplantation and research and is home to the Transplantation and Cellular Therapy Program, the Sprott Centre for Stem Cell Research and the Sinclair Centre for Regenerative Medicine..
This expertise paid off. Geneviève’s initial care team included Dr. Mitchell Sabloff, Director of the Ottawa Hospital Leukemia Program, and Hematologist Dr. Jill Fulcher. Following her stem cell transplant on March 29th, 2018, she was cared for by Dr. Natasha Kekre, who was recently named the Research Chair in Advanced Stem Cell Therapy. Dr. Kekre and extended care teams at the General Campus supported Geneviève each step of the way.
The stem cell transplant was a success, and Geneviève has been in remission ever since.
In the weeks following the transplant, Geneviève was weak and fragile, so she stayed in with her parents, who had moved into an apartment in the Ottawa area to care for her. Being at home with her husband and children would have been dangerous for Geneviève, since her immune system was still recovering after the stem cell transplant.
Being apart was difficult, but she was fortunate to be in loving care of parents. With their help, she regained the strength she needed for this next step to healing.
“We wanted to show how thankful we were for what they had done, their kindness and sensitivity in all the care they provided me … My heart was filled with gratitude.”
— Geneviève Gratton
“On the 100th day after my stem cell transplant, since I had passed the darkest period of my life, my mother and I brought two huge cakes to The Ottawa Hospital — one for the team on Module L and one for the fifth-floor team,” says Geneviève. “We wanted to show how thankful we were for what they had done, their kindness and sensitivity in all the care they provided me since January 2018. My heart was filled with gratitude.”

“We are infinitely grateful”

“We want to support the research and care efforts of the hospital and believe that even a small regular donation expresses our support of the hospital.”
— Georges Gratton
It was the lifesaving care Geneviève received at The Ottawa Hospital that inspired Georges and Jeannine to donate, and they’ve been giving ever since – each month. They want to ensure the hospital has the funds they need to continue providing expert care to patients like their daughter.
“We want to support the research and care efforts of the hospital and believe that even a small regular donation expresses our support of the hospital,” says Georges.
Their monthly donations are also a meaningful way to express their deep gratitude for seeing Geneviève beat her cancer and get back to watching her three children grow up.
“We give to say thank you for the wonderful care Geneviève received,” says Jeannine. “The Ottawa Hospital saved her life, and we are infinitely grateful.”
Geneviève is now back to work and spending time with her kids, doing the things she loves most, like reading, boating, and walks in Gatineau Park. She’s not only grateful for her health, but also making the best of each day she’s been given.







Published: July 2023
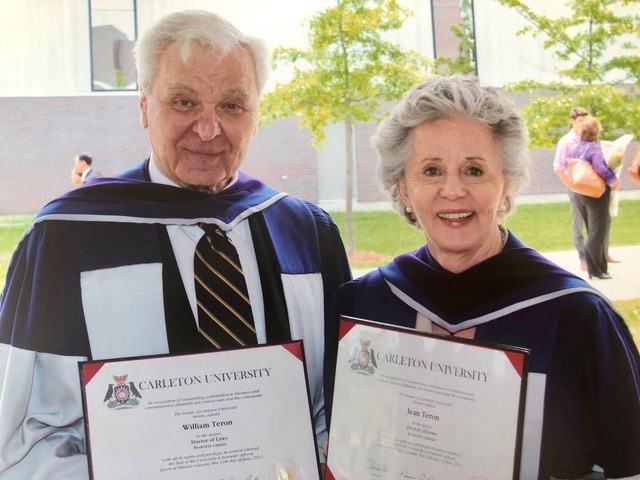
Next year, Jean Teron will proudly wear the 100-year-old nursing pin given to her mother in 1924 when she graduated — the same year the Civic Hospital opened its doors on Carling Avenue. “The Ottawa Hospital has been a lifelong part of my family,” says Jean. “My mother and sister were nurses trained there. My siblings and I and my children were born there.”
It’s that personal connection to the hospital — and to her city — that helped inspire Jean’s $100,000 gift to The Campaign to Create Tomorrow.
“The Ottawa Hospital has been a lifelong part of my family.”
— Jean Teron
But this is not the first time the Teron family has made an indelible mark on our city. Jean’s late husband, Bill Teron, was known as the “father of Kanata” for creating a small town amidst farmer’s fields and rock outcroppings west of Ottawa. What started as a dream in the 1960s became a vibrant, thriving place to call home. The Terons know better than most the importance of community.
Jean, Bill, and their family have long been supporters of The Ottawa Hospital — changing lives for decades. In 1977, Bill and Jean donated a kidney preserving machine that allowed surgeons to store and preserve kidneys for up to 40 hours while they matched kidneys with patients on a waitlist. In the years since, they helped build the Dr. Chris Carruthers Operating Room with Jean leading the way as Chair of the $1-million campaign. She was also part of The Ottawa Hospital Foundation’s Gala committee for years, helping raise funds for research. Together, the Terons contributed to the Legacy Campaign, the Centre for Stem Cell and Gene Therapy, and to fundraising efforts for the hospital through Tamarack Ottawa Race Weekend.

Jean’s daughter, Kim Teron, has also been actively involved with Partners Investing in Parkinson’s Research (PIPR) since 2011, when Kim’s husband Ross was diagnosed with Parkinson’s disease. Jean and other family members have rallied behind Kim who has worked tirelessly to raise funds and awareness for this cause.
It’s clear the Teron family is determined to make a difference.

Now, Jean’s generous gift will play a vital role in propelling The Campaign to Create Tomorrow forward, helping forge a brighter future for the community she loves by advancing medical research, expanding state-of-the-art facilities, and transforming patient care.
“As one citizen, it’s important to me that individuals and businesses in Ottawa give to this campaign to show how much the community supports the building of a great new hospital.”
— Jean Teron
Jean hopes her gift will help ignite a spark, inspiring others to follow her lead. “As one citizen, it’s important to me that individuals and businesses in Ottawa give to this campaign to show how much the community supports the building of a great new hospital,” she says. “I do hope that when people see lists of those who have donated, they too will be encouraged to participate.”







We’re thrilled to announce that The Ottawa Hospital Auxiliary has once again made a significant contribution to patient care at our hospital with a recent $1-million donation. This gift will be used to purchase 14 Philips MX750 cardiac monitors for our hospital’s Emergency Department observation units at the Civic and General Campuses.
These monitors, which include portable capabilities, are used to track heart function and record the patient’s heart rate and rhythm. According to Dr. Guy Hébert, Head of the Department of Emergency Medicine, these devices will significantly improve the department’s ability to perform cardiac monitoring.
“Gifts like this allow us to provide the very best care to patients.”
— Dr. Guy Hébert

“The Ottawa Hospital Auxiliary fills an essential role at our hospital, and we are grateful for their support. This new equipment will allow us to properly monitor and track patients’ cardiac activity during our time observing them and caring for them in the Emergency department,” says Dr. Hébert. “Gifts like this allow us to provide the very best care to patients.”
This donation comes less than a year after their $2.5-million donation in 2022. In total, they’ve donated more than $14 million in a little over a decade, which has supported a wide range of patient needs, from emergency clothing and necessities to lifesaving equipment — even an MRI machine.
“We know the funds we provide are making a tangible difference to our hospital community.”
— Catherine Higgens
The Auxiliary has been meeting patients’ needs in one way or another for almost 125 years. Each of the hospital’s three campuses used to have their own separate auxiliary, but in 2021 they amalgamated into one unified and efficient operation and emerged from the change more determined than ever. They generate income through a variety of initiatives, including on-campus vendors and retail spaces like the Civic’s gift shop and auxiliary shop as well as the General’s Boutique.
The Auxiliary is passionate about being an “on-the-ground organization,” according to the President of their Board of Directors, Catherine Higgens and is proud to make a difference. “When we see critical equipment being purchased, patients’ immediate needs being met, or see our volunteers making a difference in someone’s day, it motivates us,” she says. “We know the funds we provide are making a tangible difference to our hospital community.”
To learn more about TOH Auxiliary’s important work at our hospital, visit www.tohauxiliary.ca
Published: June 2023
When non-Hodgkins Lymphoma returned shortly after completing six rounds of chemotherapy, 73-year-old Patrick Morris was shocked to his core.
“No one plans to get cancer. No one prepares for cancer. Receiving this diagnosis was profoundly shocking. It jolted me. It was a life-changing event,” remembers Patrick. “You realize very suddenly that the life you had before will never be the same. A cancer diagnosis humbles you.”

Patrick’s hematologist, Dr. Andrew Aw, called it “refractory cancer”, because while it had responded to chemotherapy, it started to grow again — quickly. So, Dr. Aw scheduled a new round of chemotherapy to begin immediately.
This was a challenging time for Patrick, who, up until this point in his life, was fortunate to be in good health and never one to sit idly. In fact, he enjoyed significant success as an elite ski jumper in the late 60s and early 70s, and that same drive propelled him to the top of his industry as an award-winning, Ottawa-area real estate agent with a successful brokerage, the Morris Home Team at Royal LePage Performance Realty.
Caring for his ‘soulmate’
An important part of Patrick’s success story was his wife, Susan. Vibrant, caring, and fun-loving, Susan was his business partner for years and his soulmate. She was also an outstanding mom to their three daughters and a doting “nana”. But in 2017, Susan developed Alzheimer’s and Lewy Body Dementia. Patrick cared for her 24/7, but she continued to decline and eventually required long-term care in 2021.

“The memories we shared are now my treasured souvenirs.”
– Patrick Morris
“I was lucky to have Susan as my wife, my business partner for many years, and my soulmate,” says Patrick. “Our marriage worked because it was a never-ending love story.”
While she no longer recognizes Patrick or their daughters, he remains deeply grateful for more than four decades together. “The memories we shared are now my treasured souvenirs.”
Exploring CAR T-cell therapy
As Patrick faced his own health challenges, it would seem the cancer was not backing down. During his second series of treatments, he received yet another shock – the cancer had spread to his lower neck. Dr. Aw was concerned, but he had a plan — one that would ultimately save Patrick’s life.


“Dr. Aw told me ‘We cannot let this get to your brain.’ And that’s when we stopped the second chemo treatment, and he recommended daily radiation.” Then, Dr. Aw explored whether Patrick was eligible for CAR T-cell therapy.
This revolutionary therapy uses the patient’s own immune cells, known as T-cells, to treat their cancer. T-cells play a critical role in the immune system by killing abnormal cells, but sometimes, cancerous cells can hide from the T-cells that are meant to kill them. However, with CAR-T therapy, those T-cells are collected and reprogrammed in the lab to be able to recognize the cancerous cells. These reprogrammed cells are then infused back into the patient, where they multiply by the millions to attack and kill the cancer.
“Every doctor, nurse, physiotherapist — everyone associated with my CAR T-cell therapy — was determined to see me have a future.”
– Patrick Morris
Patrick’s T-cells were sent to the United States for reprogramming, but researchers at The Ottawa Hospital, working with colleagues in BC, have developed the first made-in-Canada CAR-T therapy. This approach is enabling more equitable access to CAR-T therapy across the country, while also fueling groundbreaking research into better CAR-T therapies that may work for more kinds of cancer. This kind of research is possible because of the hospital’s world-class research facilities and resources, including the Biotherapeutics Manufacturing Centre and Ottawa Methods Centre.
Cancer treatment delivers knockout punch
For Patrick, CAR T-cell therapy proved to be a knockout punch for the lymphoma. Since receiving the treatment in November 2022, Patrick’s scans show no signs of cancer.
“The CAR T-cell therapy saved my life. I am in remission and have a future.”
– Patrick Morris
“When you’re faced with your own mortality, it impacts your life forever. You want the finest medical science and practitioners on your side,” says Patrick. “As an inpatient, I witnessed firsthand the dedication, commitment, and devotion of every healthcare worker. Every doctor, nurse, physiotherapist — everyone associated with my CAR T-cell treatment — was determined to see me have a future.”
The support he received from his care team was mirrored by his family and community, who, as Patrick is quick to point out, are also affected when a loved one is diagnosed with cancer. “My daughters in Ottawa were my angels on the ground. They put hundreds of kilometres on their cars, driving me back and forth to the Cancer Centre and ensuring I was cared for at home,” recalls Patrick. “My youngest daughter who lives out of town was in constant communication with me, and if she lived here, she would have shared the responsibility of support. My siblings and relatives were huge cheerleaders. My neighbours, friends, and business colleagues were rooting for me every day. There were so many helpful and supportive people. It helped me remain positive especially during the most difficult hours.”


Deep gratitude leads to first-time donation
Never far from Patrick’s mind while battling lymphoma was Susan and what she would say to him if she were able. “I know that I must look to the future. That is something my wife would say to me, and she would insist that I listen to her,” says Patrick. “It makes me smile because when I listened to Susan, she was usually correct.”
With the future in mind, and to show his gratitude, Patrick decided to make a sizable first-time donation to The Ottawa Hospital of $150,000. He hopes it will inspire others to give and will help future patients benefit from the groundbreaking treatments being developed at the hospital — like the CAR-T-cell therapy he received. He is also giving his time volunteering as a table host for the hospital’s annual President’s Breakfast and rallying others to join him for the important event.
“I will be a proud donor to The Ottawa Hospital to help support the development of more research.”
– Patrick Morris
“The Ottawa Hospital is a forerunner in immunotherapy,” he says. “I will be a proud donor to help support the development of more research — because more research produces more discoveries. CAR T-cell therapy saved my life. I am in remission and have a future.”
June 19, 2023, OTTAWA, ON – Partners with Deloitte Canada stepped forward to support the historic Campaign to Create Tomorrow in an unprecedented way. With a goal of $1 million, members of the Deloitte partner team showed their dedication and commitment to this once-in-a-generation opportunity.
Through the leadership of Mark Noonan, Vice Chair, Deloitte, and member of The Ottawa Hospital Foundation Board of Directors, the partners realized their goal. “Corporate responsibility is vitally important to further enhance our city, especially when it comes to our health. Our partners at Deloitte, along with their family members and friends, understood the need for this new hospital campus and we now encourage our peers in the industry to join us to help build the most patient-centred and technologically advanced research hospital in the country. We couldn’t be prouder to lead the way.”
With 50 partners from Deloitte’s Ottawa group participating in this special effort to support the Campaign to Create Tomorrow, Tim Kluke, President and CEO of The Ottawa Hospital Foundation said this is an excellent example of businesses coming together to reshape healthcare for future generations. “We’re deeply grateful to Mark, who led this fundraising initiative and engaged his partners. They put their hands up and each made a personal commitment to the campaign. They recognized the need to build the new hospital campus and take our research to the next level. It’s really inspiring, and I believe other community-minded businesses will follow suit.”
To join the Campaign to Create Tomorrow in support of The Ottawa Hospital, visit CreatingTomorrow.ca.
About The Ottawa Hospital:
The Ottawa Hospital is one of Canada’s top learning and research hospitals where we are guided by our vision to provide the world-class and compassionate care we would all want for our loved ones. Our multi-campus hospital, affiliated with the University of Ottawa, is home to the Regional Trauma Centre and Cancer Centre, and to new discoveries that are adopted globally to save lives.
Backed by generous support from the community, we are focused on reshaping the future of healthcare to improve the lives of our diverse population of patients from eastern Ontario, western Quebec, and Nunavut.
For more information about The Ottawa Hospital, visit OHFoundation.ca.
-30-
If there’s one word that comes to mind when you first meet Major James Morrison (Ret’d), it’s “dedication.” He is deeply dedicated to his country, his wife, and our healthcare system. It’s a loyalty that spanned decades — the major will be 100 years old in 2024. He was born the same year The Ottawa Hospital Civic campus first opened in 1924.

Every year, for the last 29 years, Major Morrison has generously donated to The Ottawa Hospital.
“I owe it to the hospital for the care they gave me.”
— Major James Morrison
When asked what motivates him to give so loyally, he answers with a charming smile. “Well, mostly because I was a customer there. And I owe it to the hospital for the care they gave me.”
First, it was heart issues. Then, ten years ago, prostate cancer.
“I was treated very well there,” he says, recounting how, at the end of his cancer treatment, he got to ring the bell not once, but eight times.
“Because that’s the Navy tradition. That’s either noon or midnight,” he explains, referring to the tradition of ringing of the ship’s bell eight times to mark the “end of watch,” or in some instances, as a nautical euphemism for finished.
Despite Major Morrison’s nod to this special tradition, it was not the Navy where he spent his long career, but the Royal Canadian Air Force, where he enlisted at just 18 years old.

“I was only 118 pounds and they said, ‘We can’t take you until you’re 120. Go home and fatten up.’ So, I went home and fattened up,” he recounts.
During the Second World War, he was posted to the Southeast Asia Air Command, and following the war, he transported prisoners to the War Crimes Trials.

Major Morrison married the love of his life, Betty, in 1951, and together they started a family. His career took them to various posts across Canada, and in 1970, he was an Officer Commanding at the Canadian Armed Forces Operation Centre in Ottawa, where he delivered instructions when the War Measures Act was invoked on October 16 of that year.
Later in life, he began patrolling public areas of the airport as the Ottawa Airport Watch, and Betty accompanied him on many of those night shifts. He made his final patrol in January 2014 — on his ninetieth birthday.
These are but a few milestones on a journey that has spanned nearly 10 decades on this earth, from the highs of first enlisting as a young man to the lows of his wife’s diagnosis with Alzheimer’s. “She doesn’t know who I am anymore.”
The two have been married 72 years, and not a day goes by that he doesn’t visit her.
It’s clear Major Morrison is loyal to the core. And while many of his stories are about the past, it’s the future he wants people in Ottawa to focus on; and he encourages others to support The Ottawa Hospital’s Campaign to Create Tomorrow.
“You should invest in this because you may need it in the future at some point.”
— Major James Morrison
The $500-million campaign is the largest in Ottawa’s history and sets in motion a vision to completely reshape healthcare by building the most technologically advanced hospital in Canada and taking groundbreaking research and innovation to unprecedented heights. And it’s something Major Morrison believes is worth supporting.
“You should invest in this because you may need it in the future at some point,” he offers as wise advice to generations that follow. “This new campus is for them.”
The new hospital is expected to open in 2028, and we would love to see Major Morrison there on opening day. “I was sort of looking forward to seeing it,” he says.
Major James Morrison, thank you for your service to our country and our community.



